

Use, Durability, and Risks for Discontinuation of Initial and Subsequent Biologics in a Large Pediatric-Onset IBD Cohort
- PMID: 36804501
- PMCID: PMC10097486
- DOI: 10.1097/MPG.0000000000003734
Use, Durability, and Risks for Discontinuation of Initial and Subsequent Biologics in a Large Pediatric-Onset IBD Cohort
Abstract
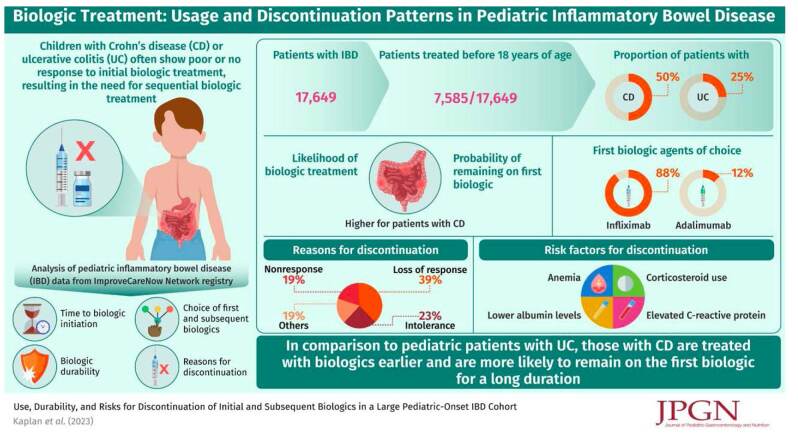
Background: Biologic medications are recommended for treatment of moderately-to-severely active Crohn disease (CD) or ulcerative colitis (UC) in children. However, many patients require sequential biologic treatment because of nonresponse or loss of response to the initial biologic.
Methods: We analyzed pediatric inflammatory bowel disease (IBD) data from the ImproveCareNow Network registry between May 2006 and September 2016, including time to biologic initiation, choice of first subsequent biologics, biologic durability, and reasons for discontinuation.
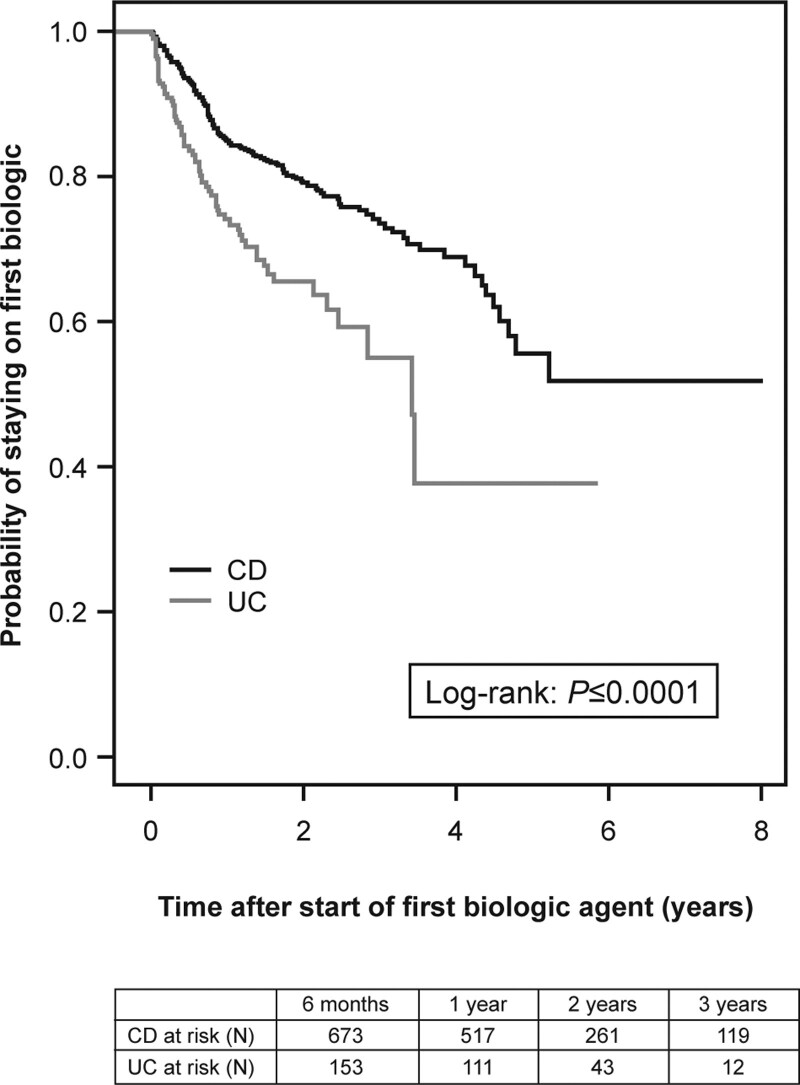
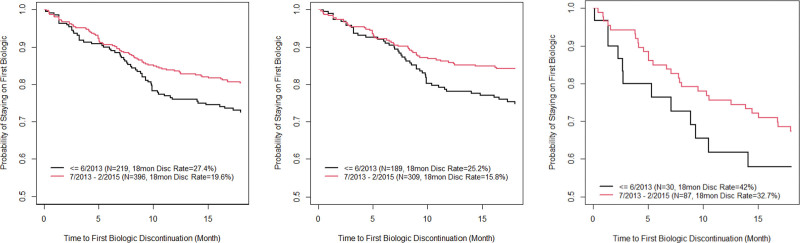
Results: Of 17,649 patients with IBD [CD: 12,410 (70%); UC: 5239 (30%)], 7585 (43%) were treated with a biologic agent before age 18 (CD: 50%; UC: 25%). Biologic treatment was more likely for CD than UC (odds ratio, 3.0; 95% CI: 2.8-3.2; P < 0.0001). First biologic agents for all patients were anti-tumor necrosis factor agents (88% infliximab, 12% adalimumab). Probability of remaining on the first biologic was significantly higher in CD than UC ( P < 0.0001). First biologics were discontinued because of loss of response (39%), intolerance (23%), and nonresponse (19%). In univariate analysis, factors associated with discontinuation of first and/or second biologics in CD include colonic-only disease, corticosteroid use, upper gastrointestinal tract involvement, and clinical and biochemical markers of severe disease. Biologic durability improved with later induction date.
Conclusions: Treatment with biologic medications is common in pediatric IBD. Patients with CD are more likely to receive biologics, receive biologics earlier in disease course, and remain on the first biologic longer than patients with UC. Multiple factors may predict biologic durability in children with IBD.
Copyright © 2023 The Author(s). Published by Wolters Kluwer on behalf of European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition.
Conflict of interest statement
R.B.C. received financial support for research in Janssen Biotech and received consultancy fees from Janssen Biotech and Janssen Research and Development. A.S.P. received lecture fee(s) from Janssen Biotech, AbbVie, and Abbott Nutrition and received consultancy fees from QOL. N.C. is an employee of Takeda Pharmaceuticals U.S.A., Inc., and owns stock or stock options. T.L. was an employee of Takeda Pharmaceuticals U.S.A., Inc., at the time the study was conducted. S.S. is in the Speaker’s Bureau for AbbVie, Inc. The remaining authors report no conflicts of interest.
Figures
References
-
- Zimmerman L, Bousvaros A. The pharmacotherapeutic management of pediatric Crohn’s disease. Expert Opin Pharmacother 2019;20:2161–8. - PubMed
-
- Bolia R, Rajanayagam J, Hardikar W, Alex G. Impact of changing treatment strategies on outcomes in pediatric ulcerative colitis. Inflamm Bowel Dis 2019;25:1838–44. - PubMed
-
- Turner D, Ruemmele FM, Orlanski-Meyer E, et al. Management of paediatric ulcerative colitis, part 1: ambulatory care—an evidence-based guideline from European Crohn’s and Colitis Organization and European Society of Paediatric Gastroenterology, Hepatology and Nutrition. J Pediatr Gastroenterol Nutr 2018;67:257–91. - PubMed
-
- AVSOLA (infliximab-axxq). Package insert. Amgen; 2019. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761086s000lbl.pdf. Accessed October 21, 2020.
-
- Remicade (infliximab). Package insert. Janssen Biotech, Inc; 2013. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/103772s5359lbl.... Accessed October 21, 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
