

Comment
doi: 10.1038/s41390-023-02493-6.
Epub 2023 Feb 17.
Band aids for Medicaid: preserving the high numbers of child health coverage during the pandemic
Collaborators,
Affiliations
- PMID: 36804503
- PMCID: PMC9937519
- DOI: 10.1038/s41390-023-02493-6
Item in Clipboard
Comment
Band aids for Medicaid: preserving the high numbers of child health coverage during the pandemic
Pediatr Res.
2023 Apr.
No abstract available
Conflict of interest statement
The author declares no competing interests.
Figures
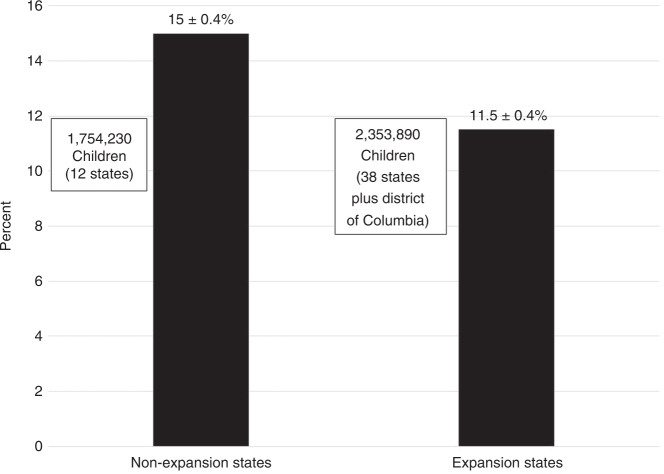
States which did not opt for Medicaid Expansion as part of the 2010 Affordable Care Act experienced higher gains in the percentage of insured children during the pandemic (mean ± standard deviation, 15 ± 0.4% vs. 11.5 ± 0.4%). While 31% of US children live in states that did not expand Medicaid, these 12 states hosted 43% of all children who gained coverage via Medicaid or CHIP during the public health emergency (data taken from ref. Appendix A, “Child Enrollment in Medicaid and CHIP by State”).
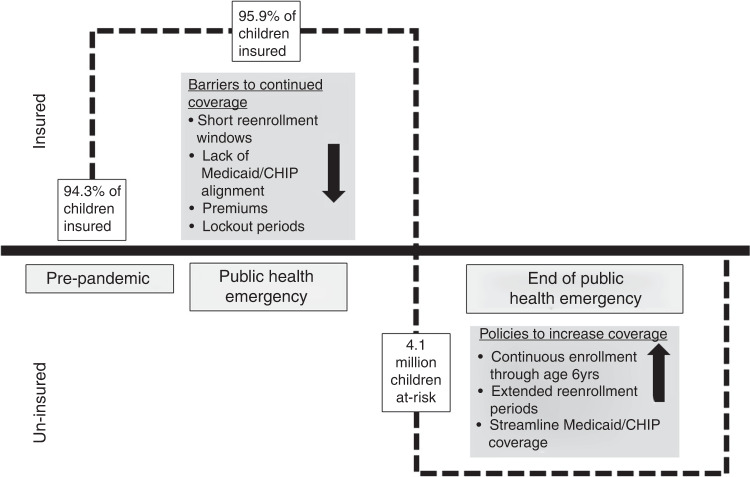
Multiple provisions impact the ability of children to continue Medicaid/CHIP coverage. Selected barriers that may reduce the number of insured children include short periods to enroll in coverage, the inability for children who lose coverage in Medicaid to be automatically enrolled in CHIP, premium payments in CHIP which hamper affordability and lockout periods during which re-enrollment is not allowed. Proposals that maintain coverage and potentially boost the percentage of insured children include continuous enrollment from birth, extended re-enrollment periods and streamlined coverage.
Comment on
-
Impaired in vivo feto-placental development is associated with neonatal neurobehavioral outcomes.Pediatr Res. 2023 Apr;93(5):1276-1284. doi: 10.1038/s41390-022-02340-0. Epub 2022 Nov 5. Pediatr Res. 2023. PMID: 36335267 Free PMC article.
References
-
- American College of Obstetricians and Gynecologists (ACOG). Fetal growth restriction: ACOG Practice Bulletin, Number 227. Obstet. Gynecol.137, e16–e28 (2021). - PubMed
