

Histologic features of allograft livers in patients treated for rejection before biopsy
- PMID: 36804507
- PMCID: PMC10121875
- DOI: 10.1016/j.humpath.2023.02.005
Histologic features of allograft livers in patients treated for rejection before biopsy
Abstract
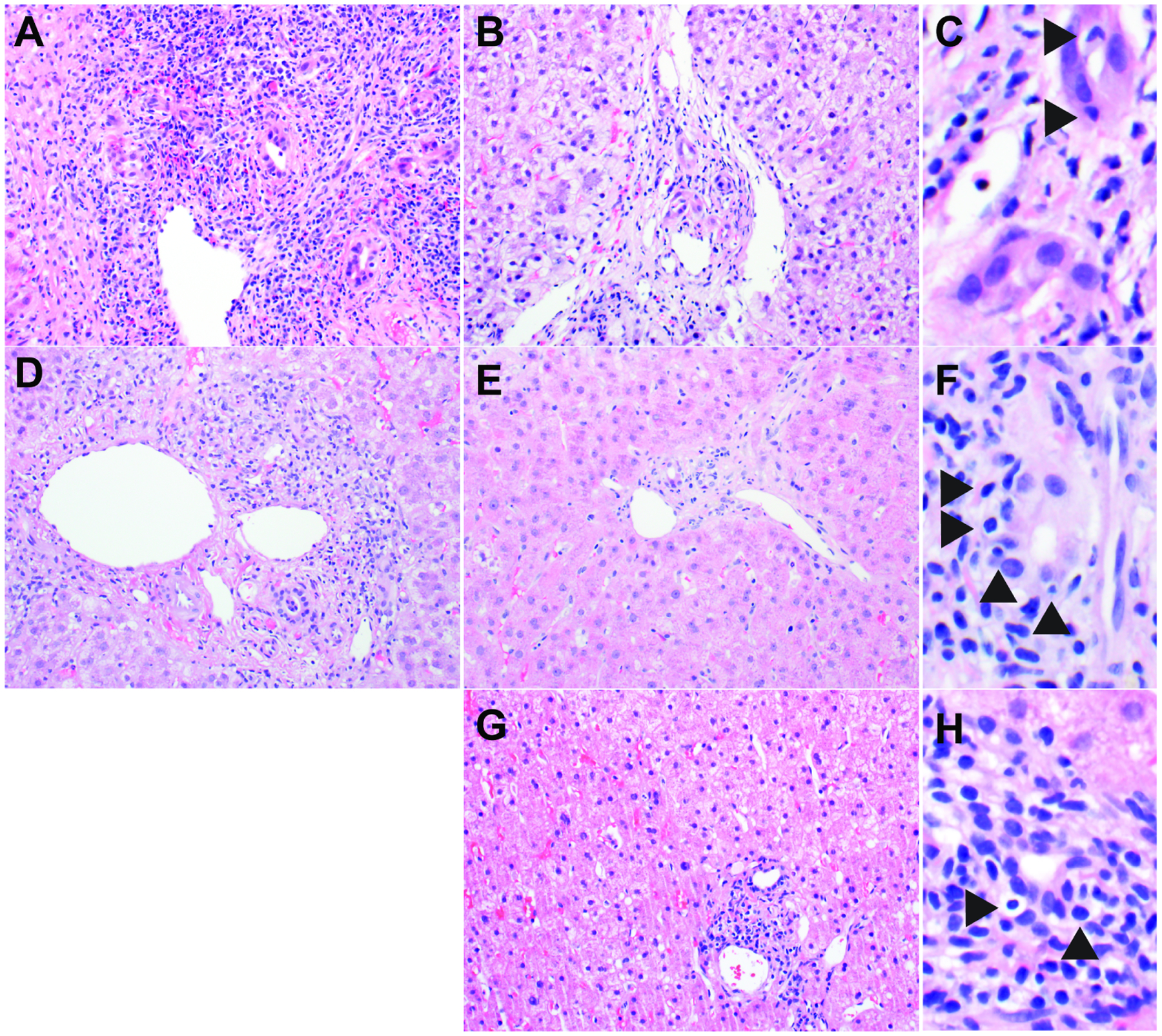
Liver biopsy is essential for management in liver transplant patients with clinical features suspicious for acute cellular rejection (ACR). As more patients are transplanted for noninfectious indications, it has become increasingly common for them to receive treatment for presumed ACR before biopsy. The effect of pretreatment on the classic histologic triad of ACR's mixed portal inflammation, endothelialitis, and bile duct damage is not well described. Here we report a retrospective study of 70 liver transplant biopsies performed on 53 patients for suspected ACR between 2018 and 2021. Thirty-seven biopsies had a clinical diagnosis of ACR after biopsy. Pretreatment with steroids, antithymocyte globulin, or other increased immunosuppression was given before biopsy in 17 of 37 cases; 20 not-pretreated cases acted as controls. A representative hematoxylin and eosin-stained slide from each biopsy was reviewed independently in a blinded fashion by 3 hepatic pathologists, graded according to the Banff system, assigned a Rejection Activity Index (RAI), and assessed for other histologic features. We found that pretreated biopsies had significantly less portal inflammation (P < .001), less endothelialitis (P < .001), lower RAI (P < .001), and less prominent eosinophils (P = .048) compared to not-pretreated biopsies. There was no significant difference for the other examined variables, including bile duct inflammation/damage (P = .32). Our findings suggest that portal inflammation and endothelialitis become less prominent with pretreatment, whereas bile duct inflammation/damage may take longer to resolve. When evaluating biopsies for suspected ACR, the finding of bile duct inflammation/damage should raise the possibility of partially treated ACR, even in the absence of endothelialitis and portal inflammation.
Keywords: Acute cellular rejection; Gastrointestinal pathology; Hepatic pathology; Liver.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no competing financial interests in relation to the work described. Potential competing interests: Shaun Chandna was a sub-investigator for Allakos. Other disclosures: Shaun Chandna has served on an advisory board for Dova Pharmaceuticals and Targeted Oncology, has served as a speaker for the Chronic Liver Disease Foundation/Focus Medical Communications, has received sponsored travel for research support from Genfit/Covance and Arrowhead Pharmaceuticals, and has received research funding from Arrowhead Pharmaceuticals, Lipocine, Calliditas Therapeutics (previously Genkyotex), and Mirum Pharmaceuticals.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
