

The optimization of postoperative radiotherapy in de novo stage IV breast cancer: evidence from real-world data to personalize treatment decisions
- PMID: 36804591
- PMCID: PMC9938892
- DOI: 10.1038/s41598-023-29888-z
The optimization of postoperative radiotherapy in de novo stage IV breast cancer: evidence from real-world data to personalize treatment decisions
Abstract
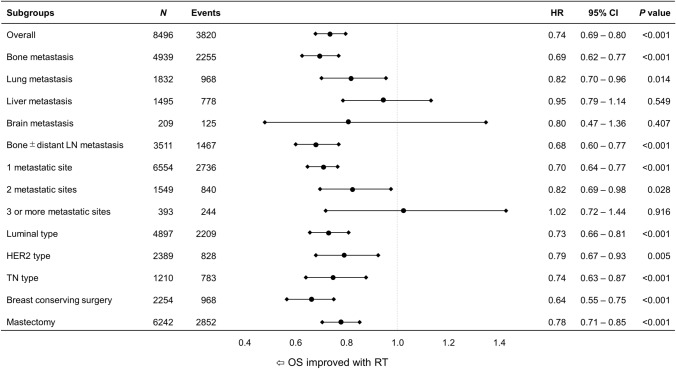
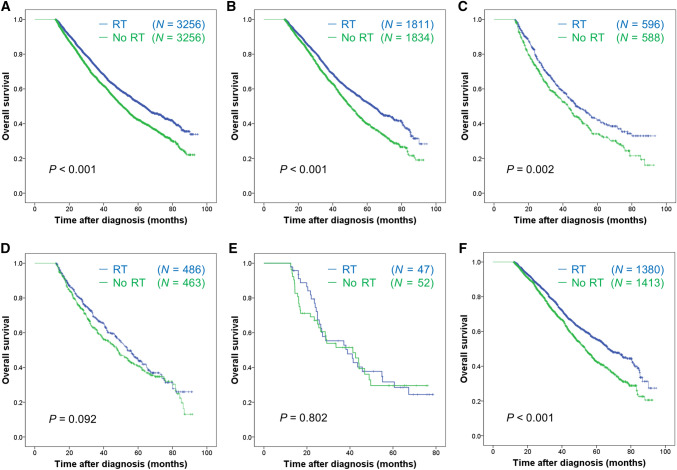
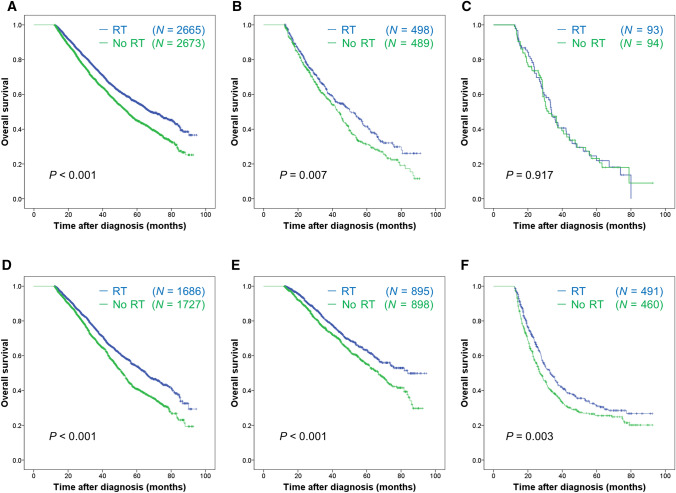
Prolonged survival of patients with stage IV breast cancer could change the role of radiotherapy for local control of breast primary, but its survival benefit remains unclear. Our aim is to investigate the survival benefit of radiotherapy in de novo stage IV breast cancer. Stage IV breast cancer patients who received breast surgery and have survived 12 months after diagnosis (landmark analysis) were included in the study from 2010 to 2015 of the National Cancer DataBase. Multivariable Cox models and a propensity score matching were used to control for confounding effects. Of 11,850 patients, 3629 (30.6%) underwent postoperative radiotherapy to breast or chest wall and 8221 (69.4%) did not. In multivariable analysis adjusting for multiple prognostic variables, postoperative radiotherapy was significantly associated with better survival (hazard ratio [HR] 0.74, 95% confidence interval [95%CI] 0.69-0.80; P < 0.001). Radiotherapy was associated with improved survival in patients with bone (P < 0.001) or lung metastasis (P = 0.014), but not in patients with liver (P = 0.549) or brain metastasis (P = 0.407). Radiotherapy was also associated with improved survival in patients with one (P < 0.001) or two metastatic sites (P = 0.028), but not in patients with three or more metastatic sites (P = 0.916). The survival impact of radiotherapy did not differ among subtypes. The results of survival analysis in the propensity score-matched sub-cohort were precisely consistent with those of multivariable analysis. These real-world data show that postoperative radiotherapy might improve overall survival for de novo Stage IV breast cancer with bone or lung metastasis, regardless of subtypes.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Postmastectomy Radiotherapy Improves Survival Benefits in De Novo Stage IV Breast Cancer: A Propensity-Score Matched Analysis.Technol Cancer Res Treat. 2022 Jan-Dec;21:15330338221089937. doi: 10.1177/15330338221089937. Technol Cancer Res Treat. 2022. PMID: 35491730 Free PMC article.
-
Survival benefit of radiotherapy after surgery in de novo stage IV breast cancer: a population-based propensity-score matched analysis.Sci Rep. 2019 Jun 12;9(1):8527. doi: 10.1038/s41598-019-45016-2. Sci Rep. 2019. PMID: 31189932 Free PMC article.
-
Additional radiotherapy to breast-conserving surgery is an optional treatment for de novo stage IV breast cancer: A population-based analysis.Cancer Med. 2021 Mar;10(5):1634-1643. doi: 10.1002/cam4.3751. Epub 2021 Feb 14. Cancer Med. 2021. PMID: 33586323 Free PMC article.
-
The Role of Surgery for Stage IV Breast Cancer.Adv Surg. 2024 Sep;58(1):293-309. doi: 10.1016/j.yasu.2024.04.016. Epub 2024 May 28. Adv Surg. 2024. PMID: 39089783 Review.
-
Locoregional treatment of de novo stage IV breast cancer in the era of modern oncology.Front Oncol. 2023 Jan 30;13:1083297. doi: 10.3389/fonc.2023.1083297. eCollection 2023. Front Oncol. 2023. PMID: 36793604 Free PMC article. Review.
Cited by
-
Axillary lymph node removal in de novo metastatic breast cancer.Gland Surg. 2024 Jul 30;13(7):1214-1228. doi: 10.21037/gs-24-130. Epub 2024 Jul 24. Gland Surg. 2024. PMID: 39175710 Free PMC article.
-
Therapeutic strategies for fungating and ulcerating breast cancers: A systematic review and narrative synthesis.Breast. 2025 Feb;79:103870. doi: 10.1016/j.breast.2024.103870. Epub 2024 Dec 30. Breast. 2025. PMID: 39862672 Free PMC article.
-
Advances in hydrogel-based materials for breast cancer bone metastasis: from targeted drug delivery to bone microenvironment remodeling.Front Pharmacol. 2025 Jun 24;16:1627883. doi: 10.3389/fphar.2025.1627883. eCollection 2025. Front Pharmacol. 2025. PMID: 40630133 Free PMC article. Review.
-
A Nomogram and Risk Classification System Predicting the Prognosis of Patients with De Novo Metastatic Breast Cancer Undergoing Immediate Breast Reconstruction: A Surveillance, Epidemiology, and End Results Population-Based Study.Curr Oncol. 2023 Dec 23;31(1):115-131. doi: 10.3390/curroncol31010008. Curr Oncol. 2023. PMID: 38248093 Free PMC article. Clinical Trial.
-
Survival Impact of Postoperative Primary Area Radiotherapy on De Novo Metastatic Breast Cancer: A Retrospective Study.Technol Cancer Res Treat. 2025 Jan-Dec;24:15330338251341195. doi: 10.1177/15330338251341195. Epub 2025 May 7. Technol Cancer Res Treat. 2025. PMID: 40336251 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
