

Costs, Health Benefits, and Cost-Effectiveness of Chlamydia Screening and Partner Notification in the United States, 2000-2019: A Mathematical Modeling Analysis
- PMID: 36804917
- PMCID: PMC10184801
- DOI: 10.1097/OLQ.0000000000001786
Costs, Health Benefits, and Cost-Effectiveness of Chlamydia Screening and Partner Notification in the United States, 2000-2019: A Mathematical Modeling Analysis
Abstract
Background: Chlamydia remains a significant public health problem that contributes to adverse reproductive health outcomes. In the United States, sexually active women 24 years and younger are recommended to receive annual screening for chlamydia. In this study, we evaluated the impact of estimated current levels of screening and partner notification (PN), and the impact of screening based on guidelines on chlamydia associated sequelae, quality adjusted life years (QALYs) lost and costs.
Methods: We conducted a cost-effectiveness analysis of chlamydia screening, using a published calibrated pair formation transmission model that estimated trends in chlamydia screening coverage in the United States from 2000 to 2015 consistent with epidemiological data. We used probability trees to translate chlamydial infection outcomes into estimated numbers of chlamydia-associated sequelae, QALYs lost, and health care services costs (in 2020 US dollars). We evaluated the costs and population health benefits of screening and PN in the United States for 2000 to 2015, as compared with no screening and no PN. We also estimated the additional benefits that could be achieved by increasing screening coverage to the levels indicated by the policy recommendations for 2016 to 2019, compared with screening coverage achieved by 2015.
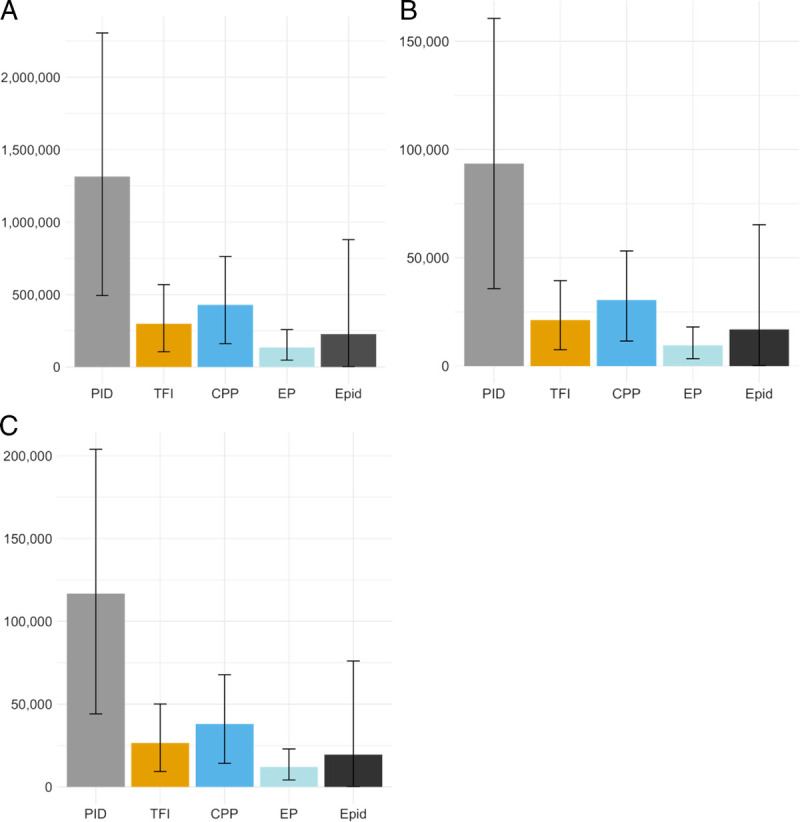
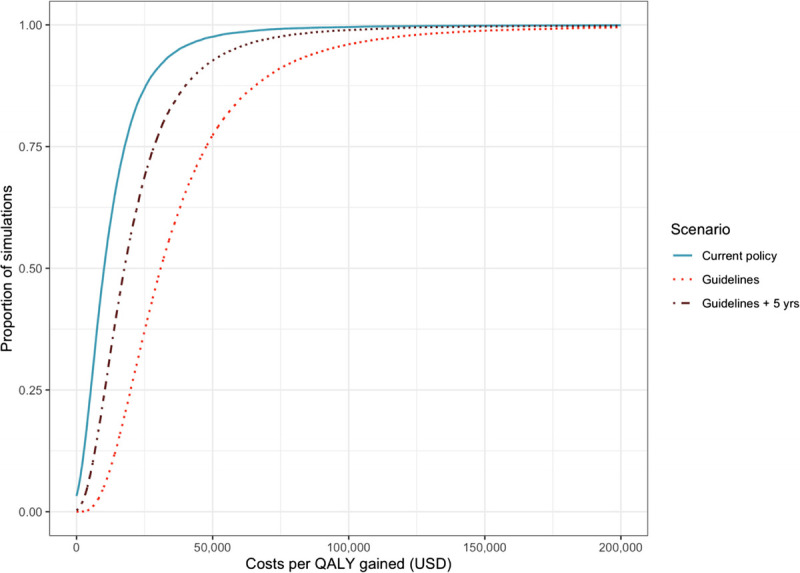
Results: Screening and PN from 2000 to 2015 were estimated to have averted 1.3 million (95% uncertainty interval [UI] 490,000-2.3 million) cases of pelvic inflammatory disease, 430,000 (95% UI, 160,000-760,000) cases of chronic pelvic pain, 300,000 (95% UI, 104,000-570,000) cases of tubal factor infertility, and 140,000 (95% UI, 47,000-260,000) cases of ectopic pregnancy in women. We estimated that chlamydia screening and PN cost $9700 per QALY gained compared with no screening and no PN. We estimated the full realization of chlamydia screening guidelines for 2016 to 2019 to cost $30,000 per QALY gained, compared with a scenario in which chlamydia screening coverage was maintained at 2015 levels.
Discussion: Chlamydia screening and PN as implemented in the United States from 2000 through 2015 has substantially improved population health and provided good value for money when considering associated health care services costs. Further population health gains are attainable by increasing screening further, at reasonable cost per QALY gained.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Sexually Transmitted Diseases Association.
Conflict of interest statement
Conflict of Interest and Sources of Funding: None declared.
Figures
Similar articles
-
Impact and cost-effectiveness of chlamydia testing in Scotland: a mathematical modelling study.Theor Biol Med Model. 2015 Jan 15;12:2. doi: 10.1186/1742-4682-12-2. Theor Biol Med Model. 2015. PMID: 25588390 Free PMC article.
-
Screening for Chlamydia trachomatis in women 15 to 29 years of age: a cost-effectiveness analysis.Ann Intern Med. 2004 Oct 5;141(7):501-13. doi: 10.7326/0003-4819-141-7-200410050-00006. Ann Intern Med. 2004. PMID: 15466767
-
The cost and cost-effectiveness of opportunistic screening for Chlamydia trachomatis in Ireland.Sex Transm Infect. 2012 Apr;88(3):222-8. doi: 10.1136/sextrans-2011-050067. Epub 2012 Jan 2. Sex Transm Infect. 2012. PMID: 22213681
-
Chlamydia trachomatis: impact on human reproduction.Hum Reprod Update. 1999 Sep-Oct;5(5):433-47. doi: 10.1093/humupd/5.5.433. Hum Reprod Update. 1999. PMID: 10582782 Review.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.Health Technol Assess. 2007 Mar;11(8):iii-iv, ix-xii, 1-165. doi: 10.3310/hta11080. Health Technol Assess. 2007. PMID: 17311735 Review.
Cited by
-
Economic Outcomes of Disease Intervention Specialist-Delivered Interventions for Sexually Transmitted Infections: A Systematic Review.Sex Transm Dis. 2025 Sep 1;52(9):511-517. doi: 10.1097/OLQ.0000000000002160. Epub 2025 Mar 14. Sex Transm Dis. 2025. PMID: 40085437
-
Follicular Fluid Metabolomics: Tool for Predicting IVF Outcomes of Different Infertility Causes.Reprod Sci. 2025 Apr;32(4):921-934. doi: 10.1007/s43032-024-01664-y. Epub 2024 Aug 1. Reprod Sci. 2025. PMID: 39090336 Free PMC article. Review.
-
Impact of a potential Chlamydia vaccine in the USA: mathematical modelling analyses.BMJ Public Health. 2024 Jan 31;2(1):e000345. doi: 10.1136/bmjph-2023-000345. eCollection 2024 Jun. BMJ Public Health. 2024. PMID: 40018092 Free PMC article.
-
Vaccination as a strategy for Chlamydia trachomatis control: a global mathematical modeling analysis.BMC Glob Public Health. 2025 Jul 25;3(1):65. doi: 10.1186/s44263-025-00181-7. BMC Glob Public Health. 2025. PMID: 40708051 Free PMC article.
-
Unveiling the Cost-Effectiveness of Chlamydia Screening Strategies: A Systematic Review.Port J Public Health. 2024 Nov 19;43(1):47-58. doi: 10.1159/000542685. eCollection 2025 Mar. Port J Public Health. 2024. PMID: 40171509 Free PMC article. Review.
References
-
- Centers for Disease Control and Prevention . Sexually Transmitted Disease Surveillance, 2020. Available at: https://www.cdc.gov/std/statistics/2020/default.htm. Accessed October 8, 2021.
-
- Rönn MM Tuite AR Menzies NA, et al. . The impact of screening and partner notification on chlamydia prevalence and numbers of infections averted in the United States, 2000–2015: Evaluation of epidemiologic trends using a pair-formation transmission model. Am J Epidemiol 2019; 188:545–554. - PMC - PubMed
-
- LeFevre ML, U.S. Preventive Services Task Force . Screening for chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2014; 161:902–910. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
