

Hypertensive emergencies and urgencies: a preliminary report of the ongoing Italian multicentric study ERIDANO
- PMID: 36805031
- PMCID: PMC9940066
- DOI: 10.1038/s41440-023-01232-y
Hypertensive emergencies and urgencies: a preliminary report of the ongoing Italian multicentric study ERIDANO
Abstract
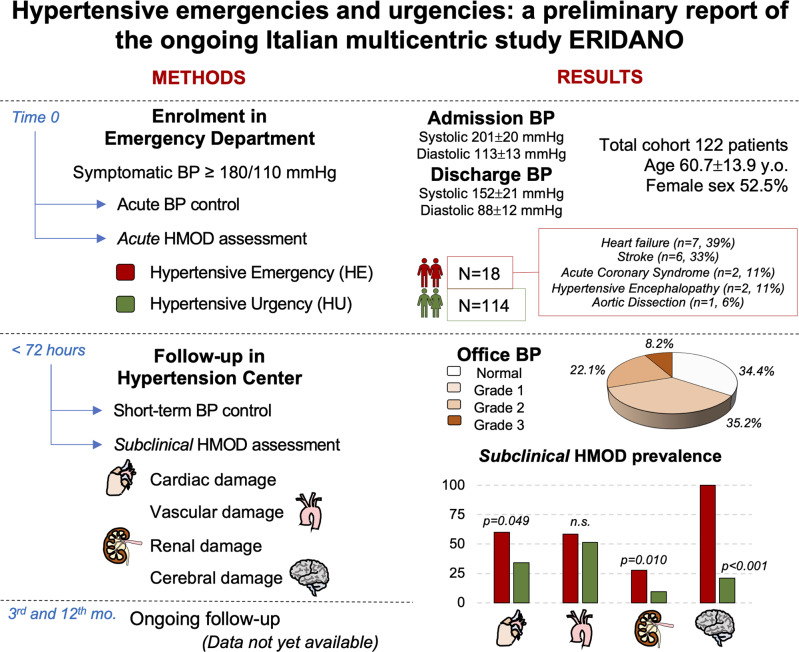
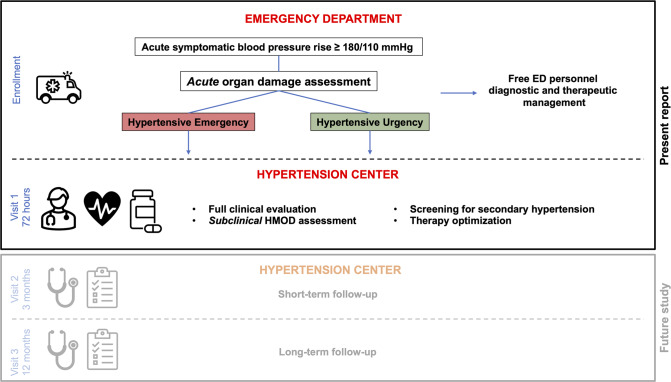
Hypertensive urgencies (HU) and hypertensive emergencies (HE) are challenges for the Emergency Department (ED). A prospective multicentre study is ongoing to characterize patients with acute hypertensive disorders, prevalence of subclinical hypertension-mediated organ damage (HMOD), short- and long-term prognosis; this is a preliminary report. Patients admitted to the ED with symptomatic blood pressure (BP) ≥180/110 mmHg were enrolled. They were managed by ED personnel according to their clinical presentations. Subsequently they underwent clinical evaluation and subclinical HMOD assessment at a Hypertension Centre within 72 h from enrolment. 122 patients were included in this report. Mean age was 60.7±13.9 years, 52.5% were females. 18 (14.8%) patients were diagnosed with HE, 108 (88.5%) with HU. There were no differences in gender, BMI, and cardiovascular comorbidities between groups. At ED discharge, 66.7% and 93.6% (p = 0.003) of HE and HU patients, respectively, had BP < 180/110 mmHg. After 72 h, 34.4% of patients resulted normotensive; 35.2%, 22.1%, and 8.2% had hypertension grade 1, 2, and 3, respectively. Patients with uncontrolled BP at office evaluation had higher vascular HMOD (49.1 vs. 25.9%, p = 0.045). Cardiac (60 vs. 34%, p = 0.049), renal (27.8 vs. 9.6%, p = 0.010) and cerebral (100 vs. 21%, p < 0.001) HMOD was more frequent in HE compared to HU group. HE showed greater cardiac, renal, and cerebral subclinical HMOD, compared to HU. 72-hours BP control is not associated with different HMOD, except for vascular HMOD; therefore, proper comprehensive examination after discharge from the ED could provide added value in cardiovascular risk stratification of such patients. One third of patients with acute blood pressure rise evaluated to the ED resulted normotensive at office evaluation (<72 hours after discharge). Patients with hypertensive emergency showed greater cardiac, renal, and cerebral subclinical HMOD, compared to the patients with hypertensive urgency. BP: blood pressure; HMOD: hypertension-mediated organ damage; y.o.: years old; mo.: months.
Keywords: emergency department; hypertension mediated organ damage; hypertensive emergencies; hypertensive urgencies; short-term blood pressure control.
© 2023. The Author(s), under exclusive licence to The Japanese Society of Hypertension.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Preliminary results of an ongoing multicentric prospective study on hypertensive emergencies and urgencies in Italy.Hypertens Res. 2023 Aug;46(8):2054-2055. doi: 10.1038/s41440-023-01341-8. Epub 2023 Jun 12. Hypertens Res. 2023. PMID: 37308554 Free PMC article.
Similar articles
-
Cardiovascular Hypertension-Mediated Organ Damage in Hypertensive Urgencies and Hypertensive Outpatients.Front Cardiovasc Med. 2022 May 16;9:889554. doi: 10.3389/fcvm.2022.889554. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35651902 Free PMC article.
-
Hypertensive emergencies and urgencies: a single-centre experience in Northern Italy 2008-2015.J Hypertens. 2020 Jan;38(1):52-58. doi: 10.1097/HJH.0000000000002213. J Hypertens. 2020. PMID: 31415308
-
Hypertensive emergencies and urgencies in emergency departments: a systematic review and meta-analysis.J Hypertens. 2020 Jul;38(7):1203-1210. doi: 10.1097/HJH.0000000000002372. J Hypertens. 2020. PMID: 32510905
-
Cardiovascular prognosis in patients admitted to an emergency department with hypertensive emergencies and urgencies.J Hypertens. 2021 Dec 1;39(12):2514-2520. doi: 10.1097/HJH.0000000000002961. J Hypertens. 2021. PMID: 34420015 Free PMC article.
-
Proposal of a Modified Classification of Hypertensive Crises: Urgency, Impending Emergency, and Emergency.Curr Vasc Pharmacol. 2024;22(3):180-186. doi: 10.2174/0115701611270174231204110557. Curr Vasc Pharmacol. 2024. PMID: 39188222 Review.
Cited by
-
Cardiac Morphology, Function, and Left Ventricular Geometric Pattern in Patients with Hypertensive Crisis: A Cardiovascular Magnetic Resonance-Based Study.J Cardiovasc Dev Dis. 2023 Aug 27;10(9):367. doi: 10.3390/jcdd10090367. J Cardiovasc Dev Dis. 2023. PMID: 37754796 Free PMC article.
-
The Role of Cardiac Biomarkers in the Diagnosis of Hypertensive Emergency.Diagnostics (Basel). 2023 Apr 30;13(9):1605. doi: 10.3390/diagnostics13091605. Diagnostics (Basel). 2023. PMID: 37174996 Free PMC article.
-
Preliminary results of an ongoing multicentric prospective study on hypertensive emergencies and urgencies in Italy.Hypertens Res. 2023 Aug;46(8):2054-2055. doi: 10.1038/s41440-023-01341-8. Epub 2023 Jun 12. Hypertens Res. 2023. PMID: 37308554 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
