

Delivery of mitochondria confers cardioprotection through mitochondria replenishment and metabolic compliance
- PMID: 36805084
- PMCID: PMC10188643
- DOI: 10.1016/j.ymthe.2023.02.016
Delivery of mitochondria confers cardioprotection through mitochondria replenishment and metabolic compliance
Abstract
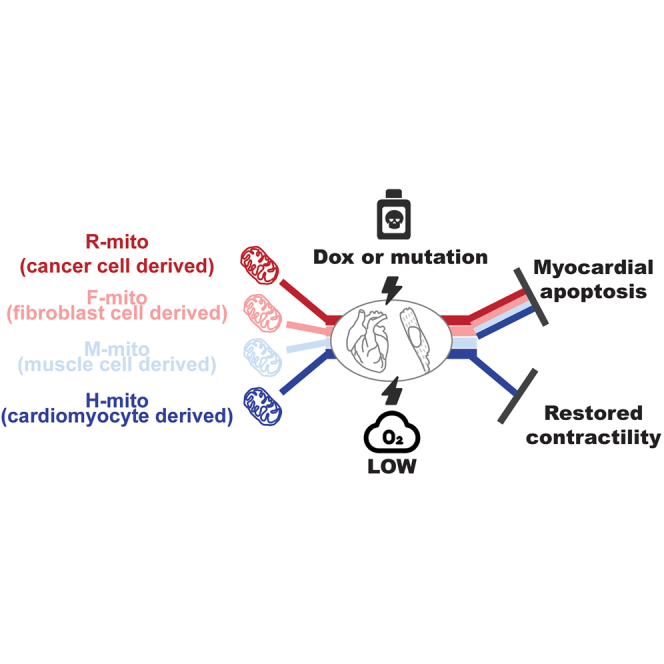
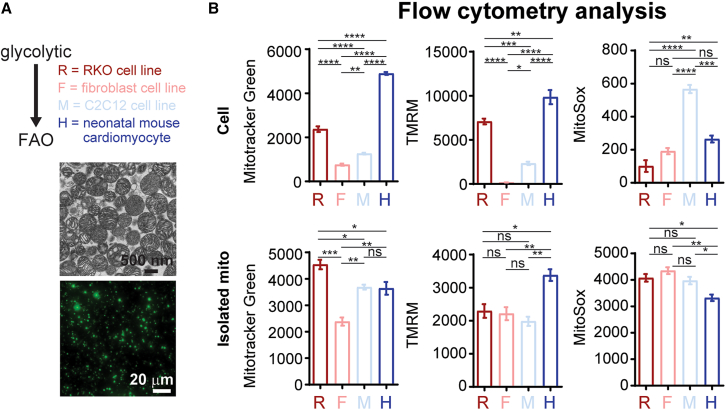
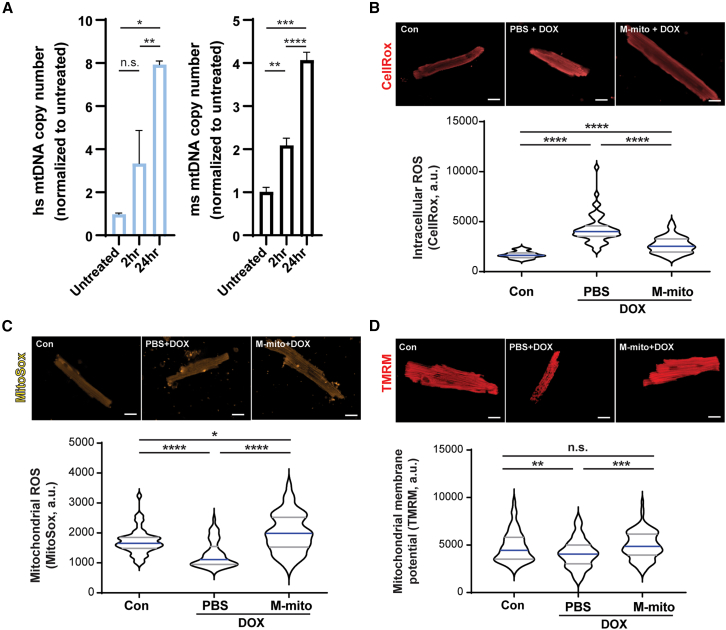
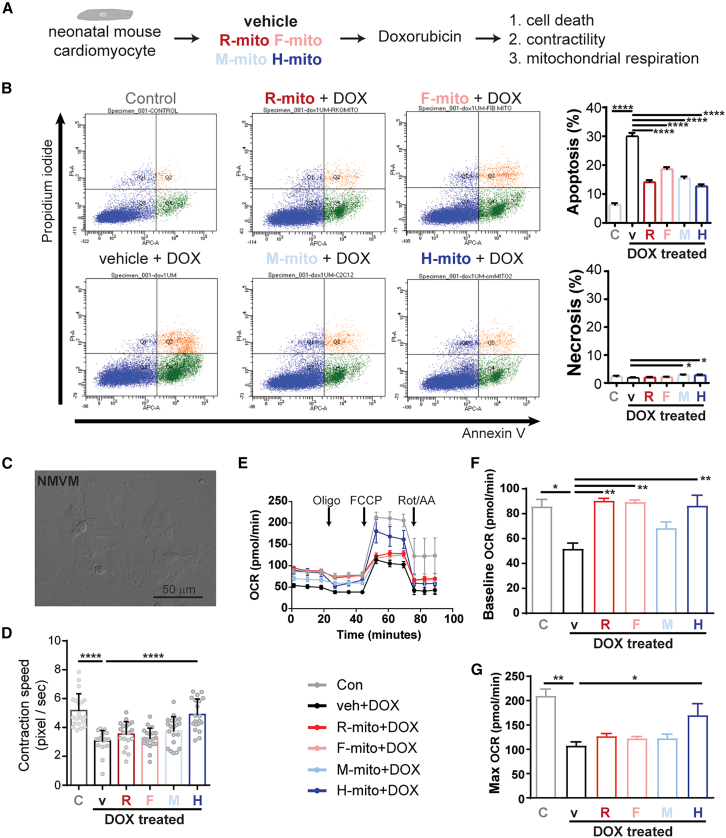
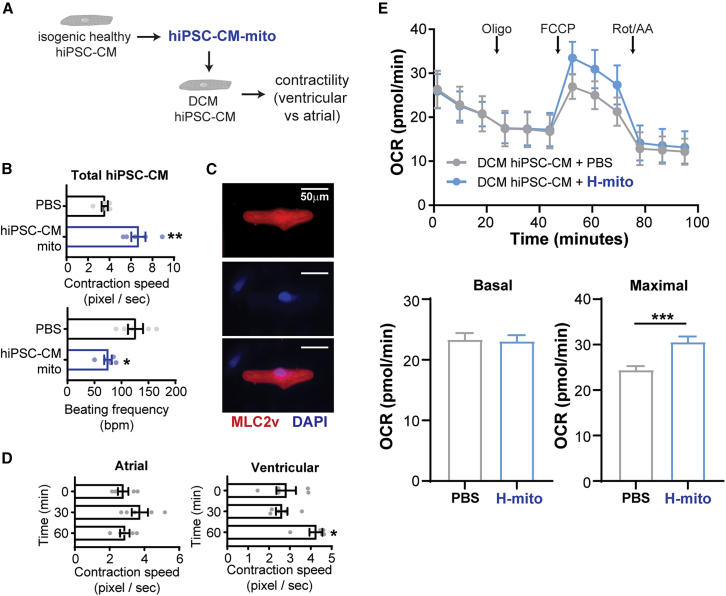
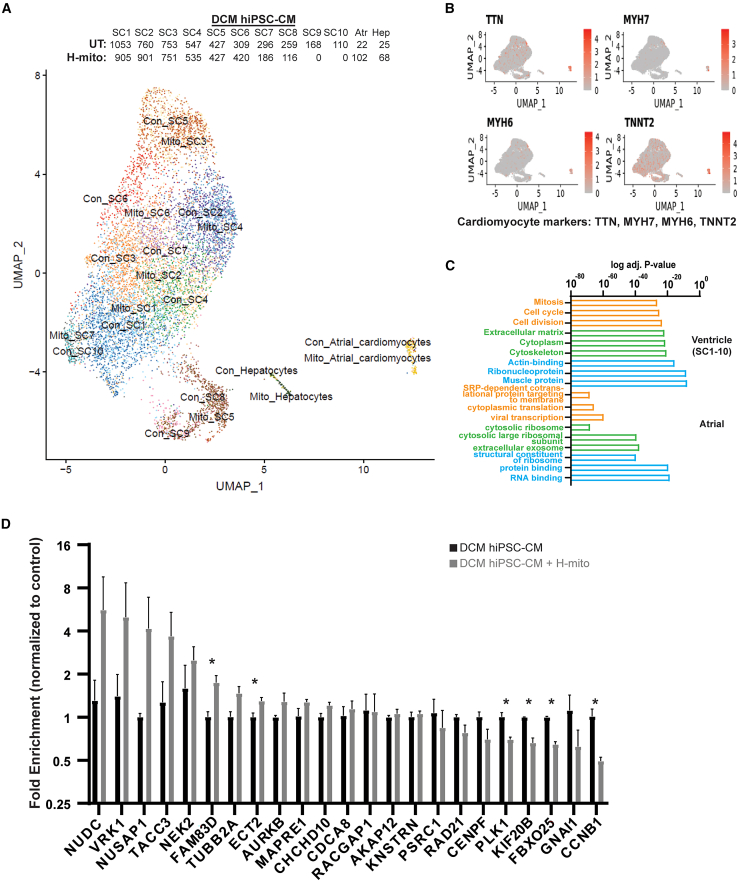
Mitochondrial dysfunction is a hallmark of heart failure. Mitochondrial transplantation has been demonstrated to be able to restore heart function, but its mechanism of action remains unresolved. Using an in-house optimized mitochondrial isolation method, we tested efficacy of mitochondria transplantation in two different heart failure models. First, using a doxorubicin-induced heart failure model, we demonstrate that mitochondrial transplantation before doxorubicin challenge protects cardiac function in vivo and prevents myocardial apoptosis, but contraction improvement relies on the metabolic compatibility between transplanted mitochondria and treated cardiomyocytes. Second, using a mutation-driven dilated cardiomyopathic human induced pluripotent stem cell-derived cardiomyocyte model, we demonstrate that mitochondrial transplantation preferentially boosts contraction in the ventricular myocytes. Last, using single-cell RNA-seq, we show that mitochondria transplantation boosts contractility in dystrophic cardiomyocytes with few transcriptomic alterations. Together, we provide evidence that mitochondria transplantation confers myocardial protection and may serve as a potential therapeutic option for heart failure.
Keywords: dilated cardiomyopathy; doxorubicin; iPSC; mitochondria delivery.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests None.
Figures
Comment in
-
Harnessing mitochondrial transplantation to sustain cardiac function: Another step forward.Mol Ther. 2023 May 3;31(5):1201-1203. doi: 10.1016/j.ymthe.2023.04.003. Mol Ther. 2023. PMID: 37141857 Free PMC article. No abstract available.
References
-
- Conrad N., Judge A., Tran J., Mohseni H., Hedgecott D., Crespillo A.P., Allison M., Hemingway H., Cleland J.G., McMurray J.J.V., et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet. 2018;391:572–580. doi: 10.1016/s0140-6736(17)32520-5. - DOI - PMC - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. James S.L., Abate D., Abate K.H., Abay S.M., Abbafati C., Abbasi N., Abbastabar H., Abd-Allah F., Abdela J., Abdelalim A., et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/s0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Virani S.S., Alonso A., Benjamin E.J., Bittencourt M.S., Callaway C.W., Carson A.P., Chamberlain A.M., Chang A.R., Cheng S., Delling F.N., et al. Heart disease and stroke statistics—2020 update: a report from the American heart association. Circulation. 2020;141:e139–e596. doi: 10.1161/cir.0000000000000757. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
