

Functional Homologous Recombination Assay on FFPE Specimens of Advanced High-Grade Serous Ovarian Cancer Predicts Clinical Outcomes
- PMID: 36805632
- PMCID: PMC10425726
- DOI: 10.1158/1078-0432.CCR-22-3156
Functional Homologous Recombination Assay on FFPE Specimens of Advanced High-Grade Serous Ovarian Cancer Predicts Clinical Outcomes
Abstract
Purpose: Deficiency in homologous recombination (HR) repair of DNA damage is characteristic of many high-grade serous ovarian cancers (HGSC). It is imperative to identify patients with homologous recombination-deficient (HRD) tumors as they are most likely to benefit from platinum-based chemotherapy and PARP inhibitors (PARPi). Existing methods measure historical, not necessarily current HRD and/or require high tumor cell content, which is not achievable for many patients. We set out to develop a clinically feasible assay for identifying functionally HRD tumors that can predict clinical outcomes.
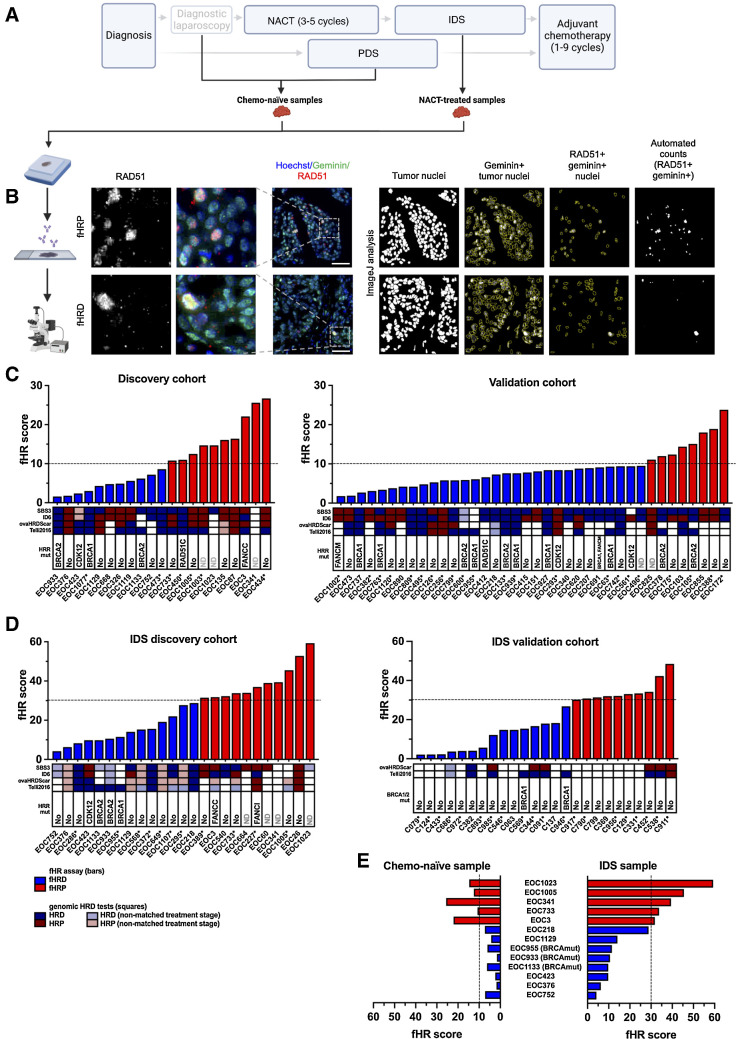
Experimental design: We quantified RAD51, a key HR protein, in immunostained formalin-fixed, paraffin-embedded (FFPE) tumor samples obtained from chemotherapy-naïve and neoadjuvant chemotherapy (NACT)-treated HGSC patients. We defined cutoffs for functional HRD separately for these sample types, classified the patients accordingly as HRD or HR-proficient, and analyzed correlations with clinical outcomes. From the same specimens, genomics-based HRD estimates (HR gene mutations, genomic signatures, and genomic scars) were also determined, and compared with functional HR (fHR) status.
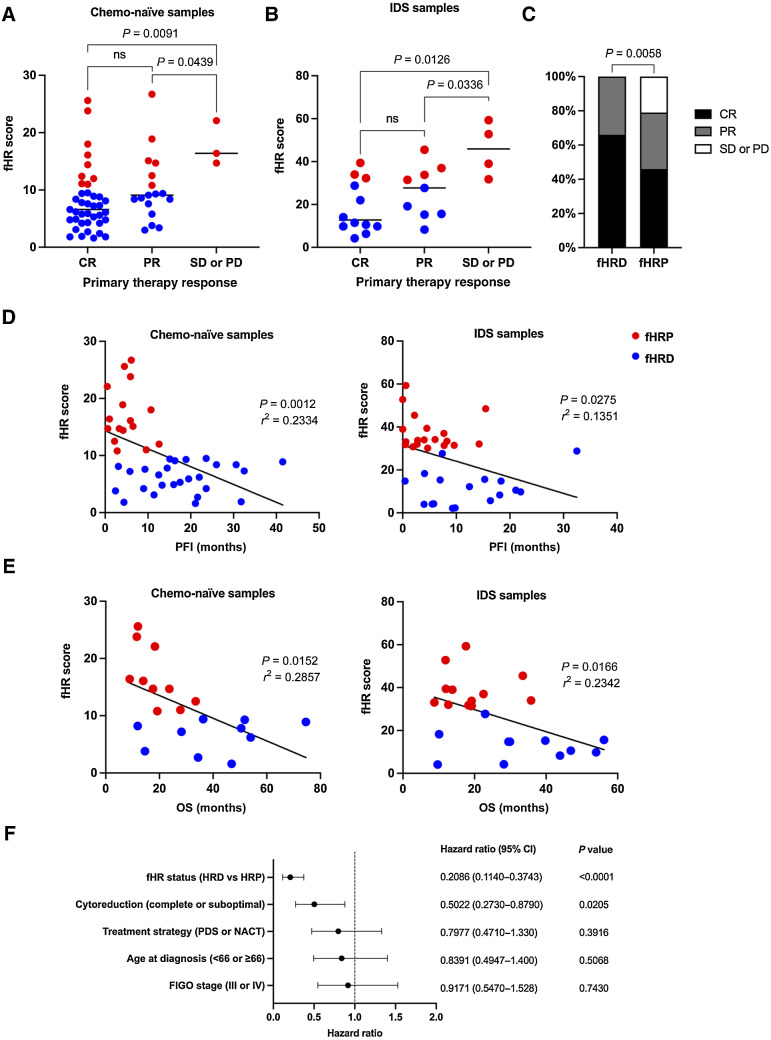
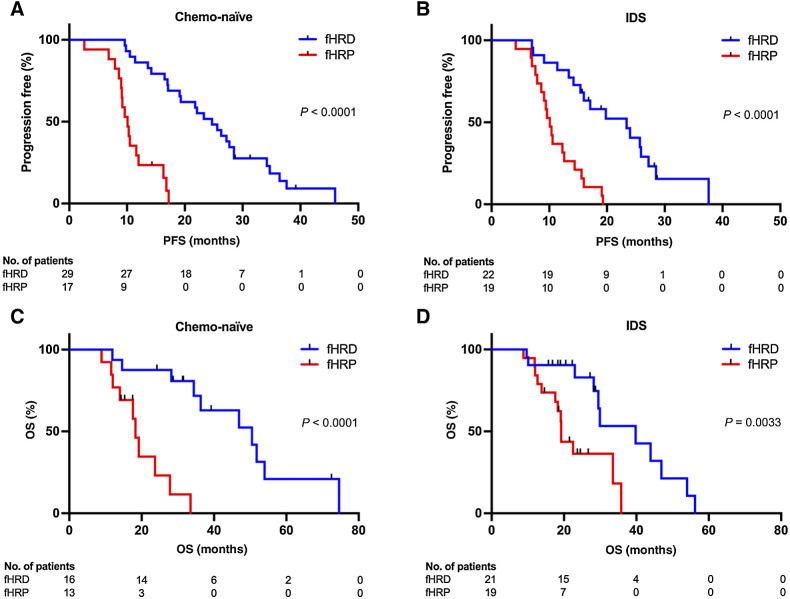
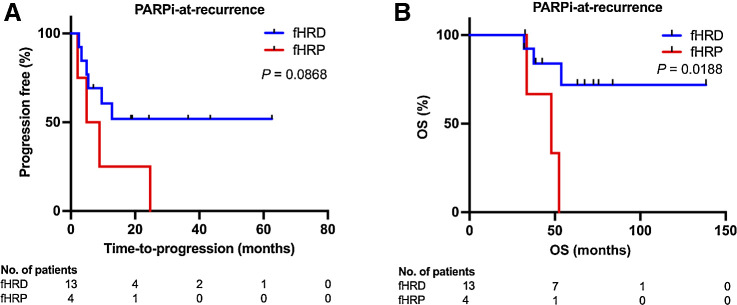
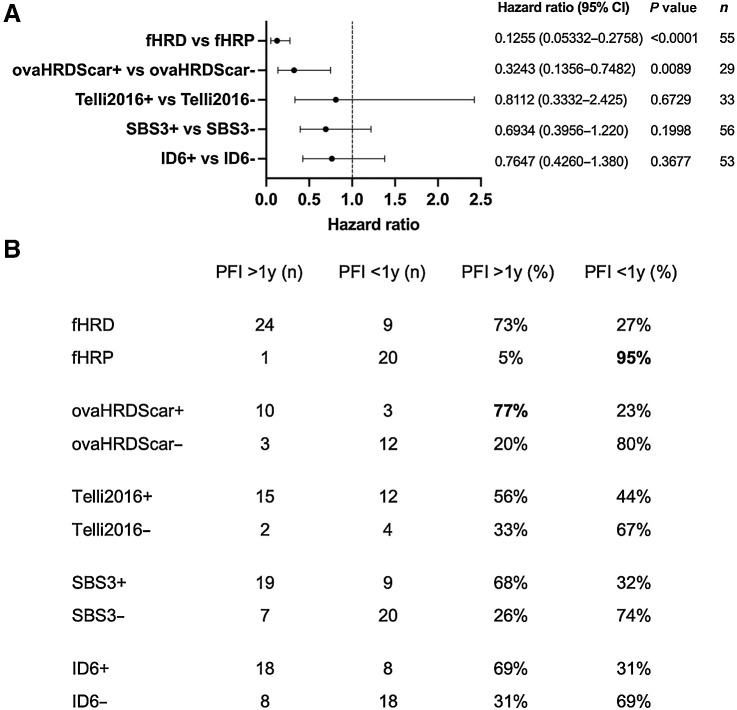
Results: fHR status significantly predicted several clinical outcomes, including progression-free survival (PFS) and overall survival (OS), when determined from chemo-naïve (PFS, P < 0.0001; OS, P < 0.0001) as well as NACT-treated (PFS, P < 0.0001; OS, P = 0.0033) tumor specimens. The fHR test also identified as HRD those PARPi-at-recurrence-treated patients with longer OS (P = 0.0188).
Conclusions: We developed an fHR assay performed on routine FFPE specimens, obtained from either chemo-naïve or NACT-treated HGSC patients, that can significantly predict real-world platinum-based chemotherapy and PARPi response. See related commentary by Garg and Oza, p. 2957.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
Assessment of Homologous Recombination Deficiency in Ovarian Cancer.Clin Cancer Res. 2023 Aug 15;29(16):2957-2960. doi: 10.1158/1078-0432.CCR-23-0563. Clin Cancer Res. 2023. PMID: 37347464
References
-
- Siddik ZH. Cisplatin: mode of cytotoxic action and molecular basis of resistance. Oncogene 2003;22:7265–79. - PubMed
-
- Farmer H, McCabe N, Lord CJ, Tutt ANJ, Johnson DA, Richardson TB, et al. . Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005;434:917–21. - PubMed
-
- Bryant HE, Schultz N, Thomas HD, Parker KM, Flower D, Lopez E, et al. . Specific killing of BRCA2-deficient tumors with inhibitors of poly (ADP-ribose) polymerase. Nature 2005;434:913–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
