

Concordance Between Initial Presumptive and Final Adjudicated Diagnoses of Infection Among Patients Meeting Sepsis-3 Criteria in the Emergency Department
- PMID: 36806551
- PMCID: PMC10273369
- DOI: 10.1093/cid/ciad101
Concordance Between Initial Presumptive and Final Adjudicated Diagnoses of Infection Among Patients Meeting Sepsis-3 Criteria in the Emergency Department
Abstract
Background: Guidelines emphasize rapid antibiotic treatment for sepsis, but infection presence is often uncertain at initial presentation. We investigated the incidence and drivers of false-positive presumptive infection diagnosis among emergency department (ED) patients meeting Sepsis-3 criteria.
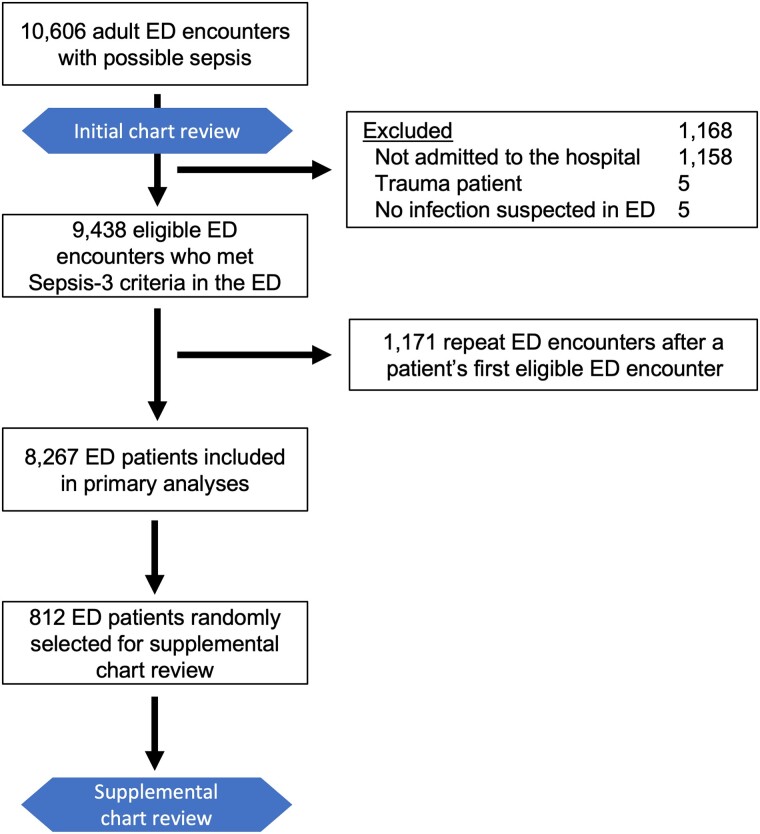
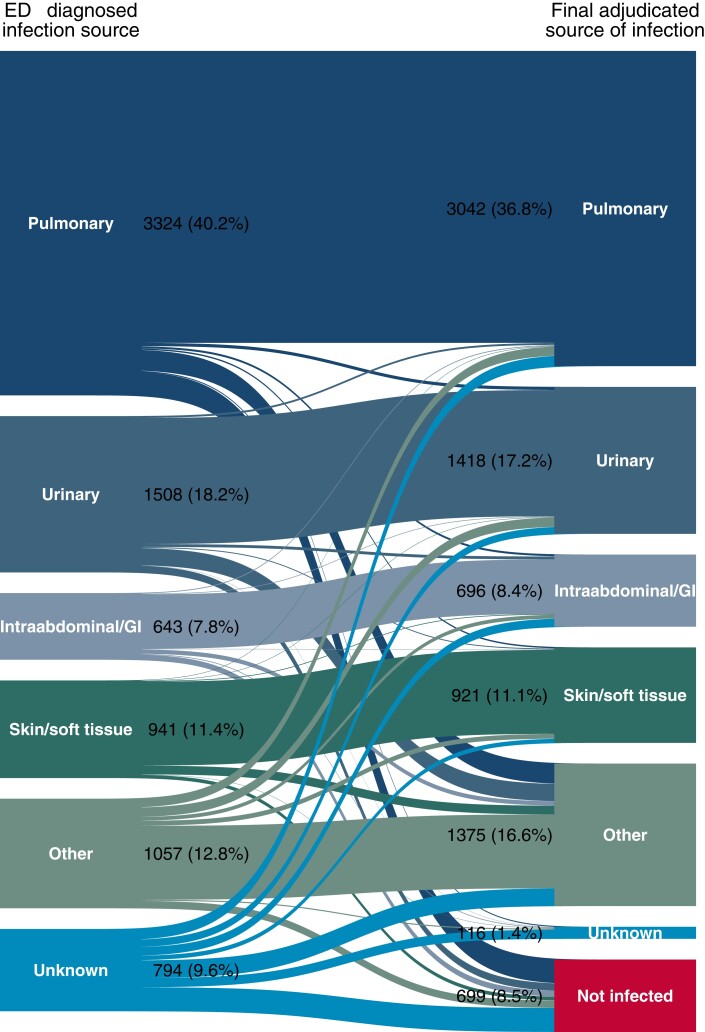
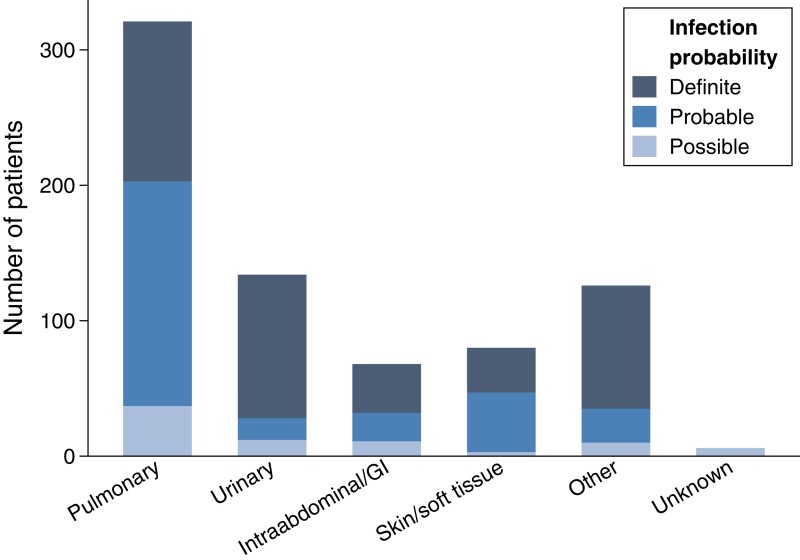
Methods: For a retrospective cohort of patients hospitalized after meeting Sepsis-3 criteria (acute organ failure and suspected infection including blood cultures drawn and intravenous antimicrobials administered) in 1 of 4 EDs from 2013 to 2017, trained reviewers first identified the ED-diagnosed source of infection and adjudicated the presence and source of infection on final assessment. Reviewers subsequently adjudicated final infection probability for a randomly selected 10% subset of subjects. Risk factors for false-positive infection diagnosis and its association with 30-day mortality were evaluated using multivariable regression.
Results: Of 8267 patients meeting Sepsis-3 criteria in the ED, 699 (8.5%) did not have an infection on final adjudication and 1488 (18.0%) patients with confirmed infections had a different source of infection diagnosed in the ED versus final adjudication (ie, initial/final source diagnosis discordance). Among the subset of patients whose final infection probability was adjudicated (n = 812), 79 (9.7%) had only "possible" infection and 77 (9.5%) were not infected. Factors associated with false-positive infection diagnosis included hypothermia, altered mental status, comorbidity burden, and an "unknown infection source" diagnosis in the ED (odds ratio: 6.39; 95% confidence interval: 5.14-7.94). False-positive infection diagnosis was not associated with 30-day mortality.
Conclusions: In this large multihospital study, <20% of ED patients meeting Sepsis-3 criteria had no infection or only possible infection on retrospective adjudication.
Keywords: misdiagnosis; overtreatment; physician practice variation; sepsis; source diagnosis discordance.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. I. D. P. and S. M. B. have received research support outside the present work from Janssen Pharmaceuticals and the National Institutes of Health (NIH) and funding to their institution from Regeneron and the Centers for Disease Control and Prevention (CDC). S. M. B. has received royalties from Oxford University Press, research support from Sedana Medical and Faron, and payment for data safety monitoring board membership from New York University and Hamilton. E. A. S. reports research support outside the present work from CDC. C. L. H. reports research support outside the present work from NIH and the American Lung Association, support for meeting attendance and travel from Stanford University and the Critical Care Clinical Trials Consortium, and payment for data safety monitoring board membership from the I-SPY-COVID trial consortium. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Comment in
-
Measuring Diagnostic Accuracy for Infection in Patients Treated for Sepsis: An Important but Challenging Exercise.Clin Infect Dis. 2023 Jun 16;76(12):2056-2058. doi: 10.1093/cid/ciad105. Clin Infect Dis. 2023. PMID: 36804679 No abstract available.
-
The Accuracy of Infection Diagnoses Among Patients Meeting Sepsis-3 Criteria in the Emergency Department.Clin Infect Dis. 2023 Jul 26;77(2):327. doi: 10.1093/cid/ciad240. Clin Infect Dis. 2023. PMID: 37092701 Free PMC article. No abstract available.
References
-
- Evans L, Rhodes A, Alhazzani W, et al. . Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med 2021; 49:e1063–e143. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
