

Tumor Mutational Burden as a Predictor of Survival with Durvalumab and/or Tremelimumab Treatment in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
- PMID: 36806911
- PMCID: PMC10233352
- DOI: 10.1158/1078-0432.CCR-22-2765
Tumor Mutational Burden as a Predictor of Survival with Durvalumab and/or Tremelimumab Treatment in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma
Abstract
Purpose: Biomarkers that predict response to immune checkpoint inhibitors (ICI) in recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC) are needed. This retrospective study assessed tumor mutational burden (TMB) and outcomes in the phase II HAWK and CONDOR and phase III EAGLE studies of durvalumab with or without tremelimumab in platinum-resistant R/M HNSCC.
Patients and methods: Tumor samples from HAWK/CONDOR (N = 153) and blood samples from EAGLE (N = 247) were analyzed for TMB. Associations with survival were evaluated for tissue TMB (tTMB) at cutoffs from 10 to 20 mutations/megabase (mut/Mb) and for blood plasma TMB (bTMB) at cutoffs from 8 to 24 mut/Mb.
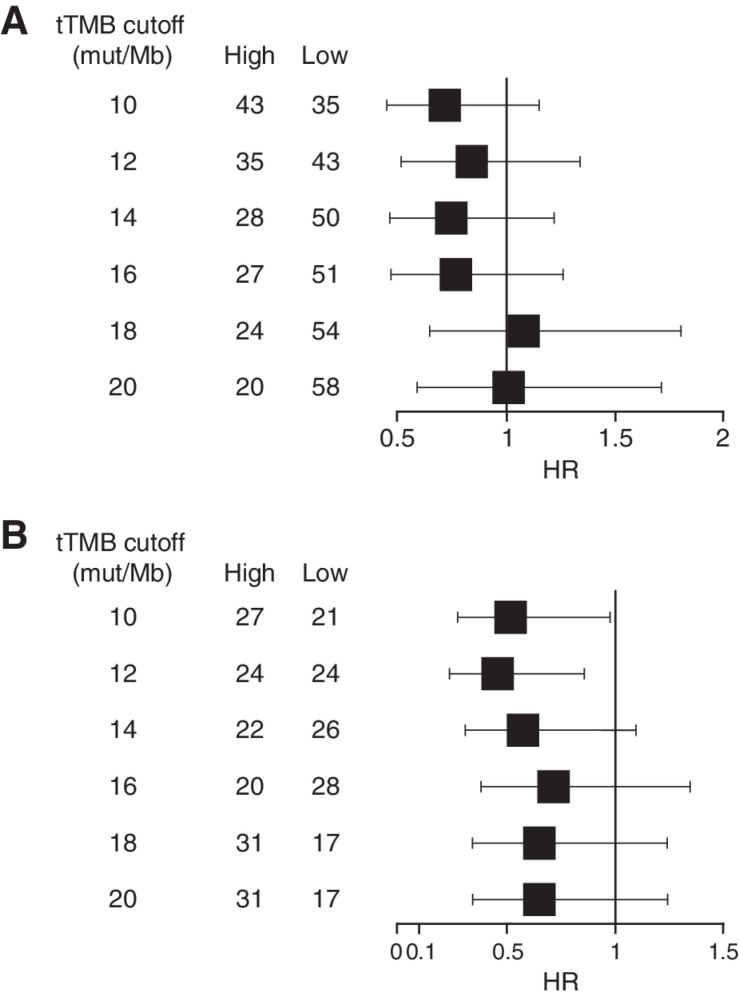
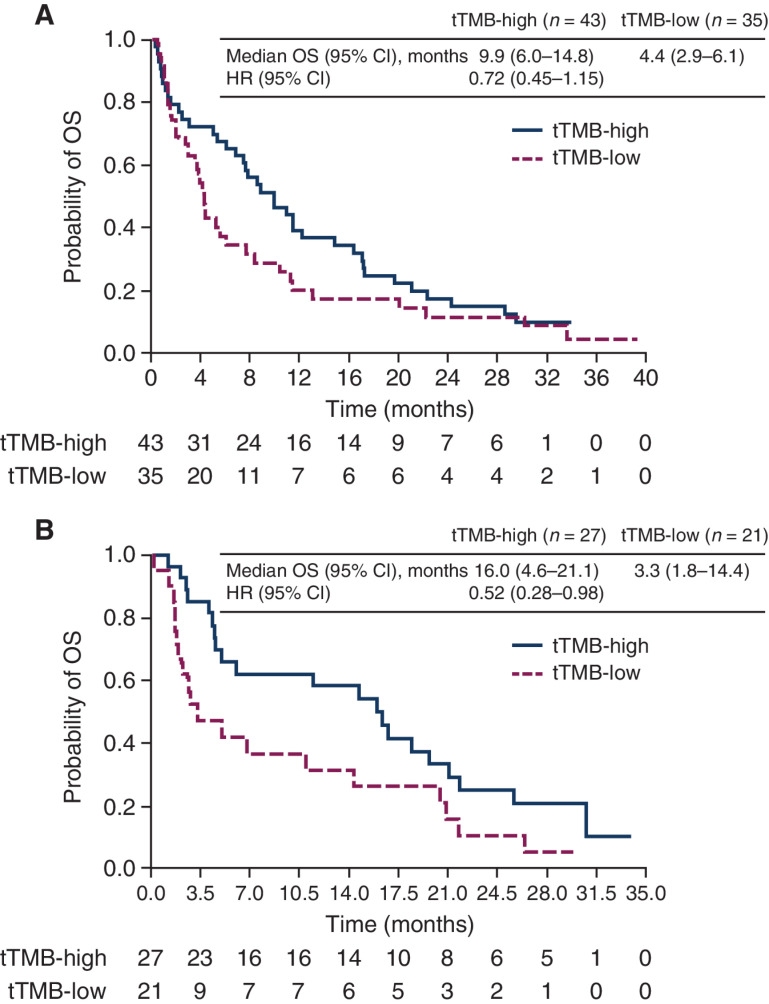
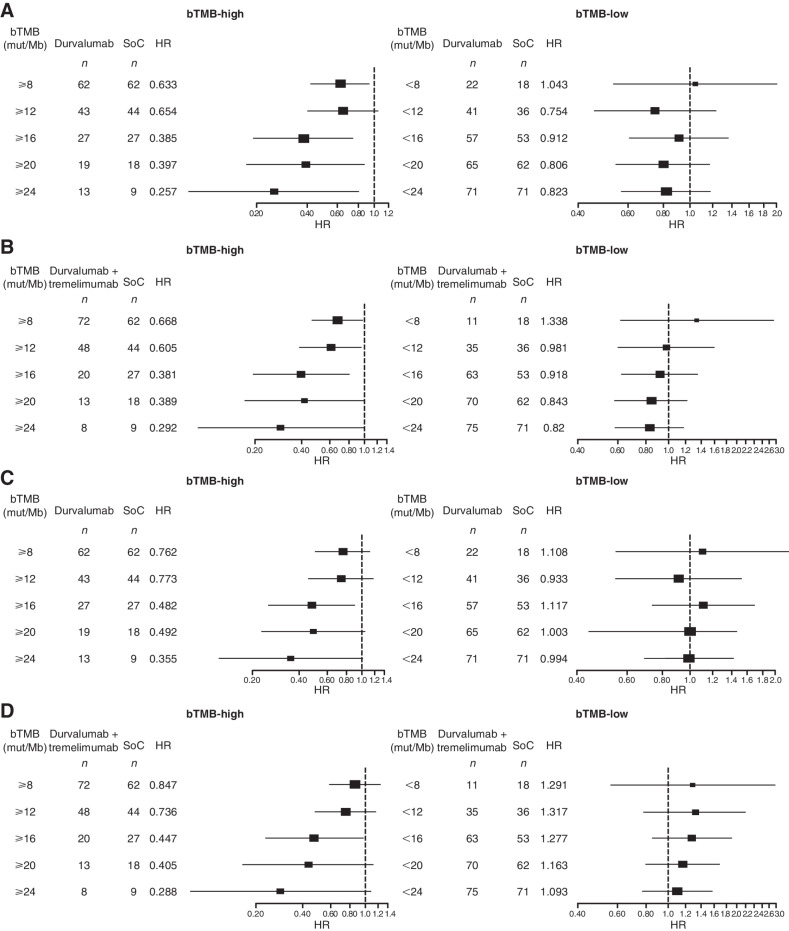
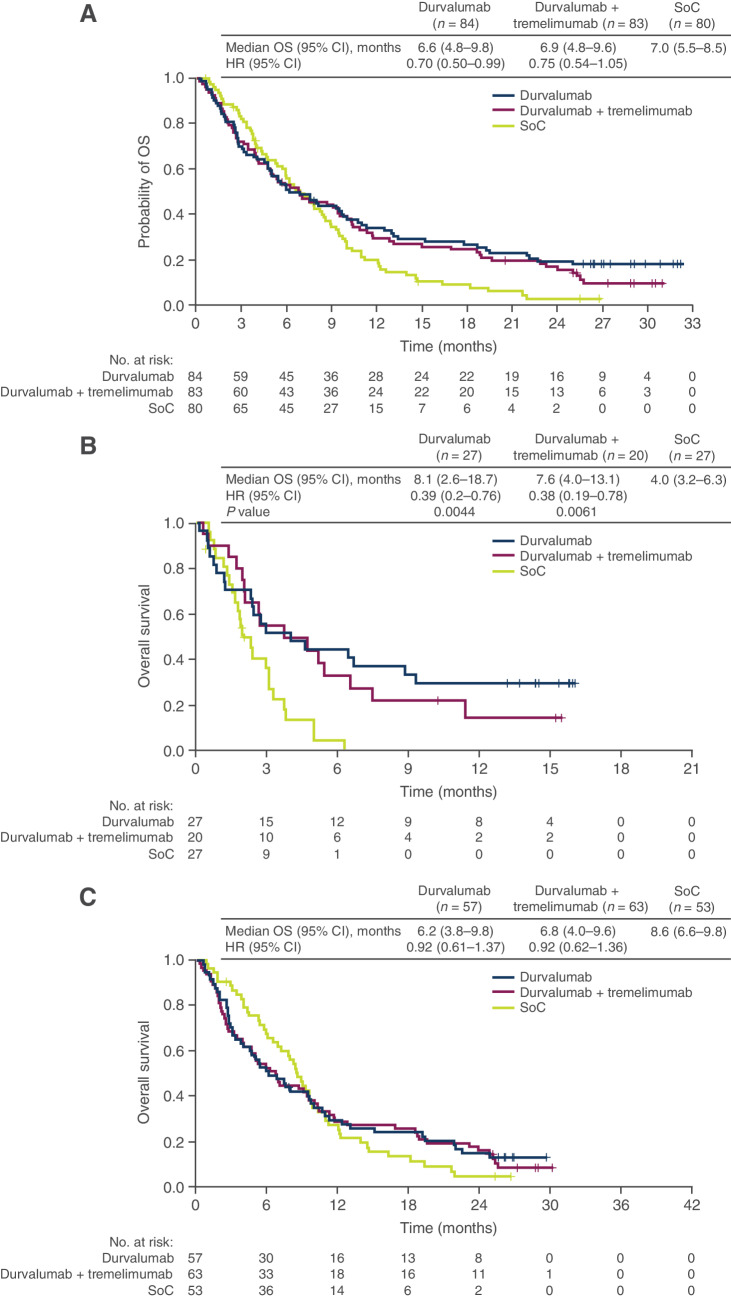
Results: In HAWK/CONDOR, overall survival (OS) with durvalumab with or without tremelimumab was longer for high versus low tTMB: statistically significant differences were observed with durvalumab plus tremelimumab at tTMB ≥ 10 mut/Mb [HR, 0.52 (95% confidence interval, CI, 0.28-0.98)] and tTMB ≥ 12 mut/Mb [HR, 0.46 (95% CI, 0.24-0.86)]. In EAGLE, a significant OS benefit versus chemotherapy was observed with durvalumab and durvalumab plus tremelimumab at bTMB≥16 mut/Mb [HR, 0.39 (95% CI, 0.20-0.76) and 0.38 (95% CI, 0.19-0.78), respectively] but not bTMB < 16 mut/Mb [HR, 0.92 (0.61-1.37) and 0.92 (95% CI, 0.62-1.36), respectively]. A significant progression-free survival benefit was also observed in the ICI arms versus chemotherapy at bTMB ≥ 16 mut/Mb.
Conclusions: Findings support TMB as a biomarker for predicting survival in patients with platinum-resistant R/M HNSCC treated with ICIs. The analysis of EAGLE demonstrated that bTMB was predictive of survival with ICI treatment versus chemotherapy in a large, randomized controlled study population.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
References
-
- Lala M, Chirovsky D, Cheng JD, Mayawala K. Clinical outcomes with therapies for previously treated recurrent/metastatic head-and-neck squamous cell carcinoma (R/M HNSCC): a systematic literature review. Oral Oncol 2018;84:108–20. - PubMed
-
- Lasinska I, Kolenda T, Teresiak A, Lamperska KM, Galus L, Mackiewicz J. Immunotherapy in patients with recurrent and metastatic squamous cell carcinoma of the head and neck. Anticancer Agents Med Chem 2019;19:290–303. - PubMed
-
- Cohen EEW, Soulières D, Le Tourneau C, Dinis J, Licitra L, Ahn MJ, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet 2019;393:156–67. - PubMed
-
- Ferris RL, Haddad R, Even C, Tahara M, Dvorkin M, Ciuleanu TE, et al. Durvalumab with or without tremelimumab in patients with recurrent or metastatic head and neck squamous cell carcinoma: EAGLE, a randomized, open-label phase III study. Ann Oncol 2020;31:942–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
