

The peripheral vascular responses in non-freezing cold injury and matched controls
- PMID: 36807667
- PMCID: PMC10103892
- DOI: 10.1113/EP090721
The peripheral vascular responses in non-freezing cold injury and matched controls
Abstract
New findings: What is the central question of this study? Does non-freezing cold injury (NFCI) alter normal peripheral vascular function? What is the main finding and its importance? Individuals with NFCI were more cold sensitive (rewarmed more slowly and felt more discomfort) than controls. Vascular tests indicated that extremity endothelial function was preserved with NFCI and that sympathetic vasoconstrictor response might be reduced. The pathophysiology underpinning the cold sensitivity associated with NFCI thus remains to be identified.
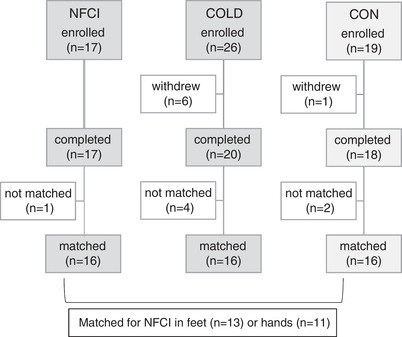
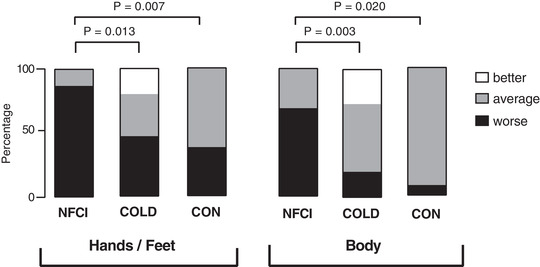
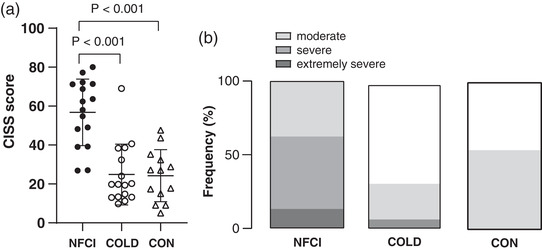
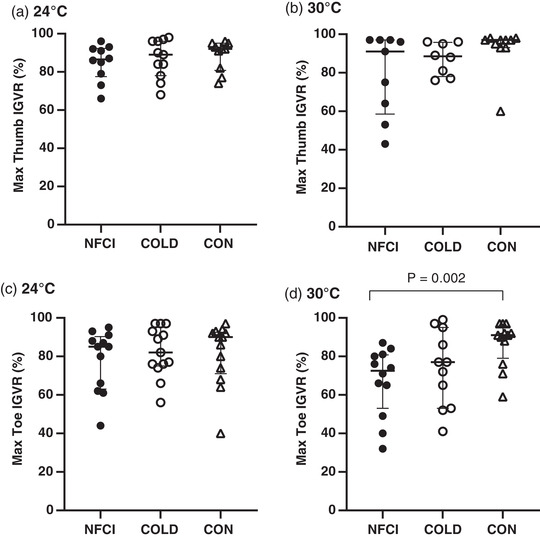
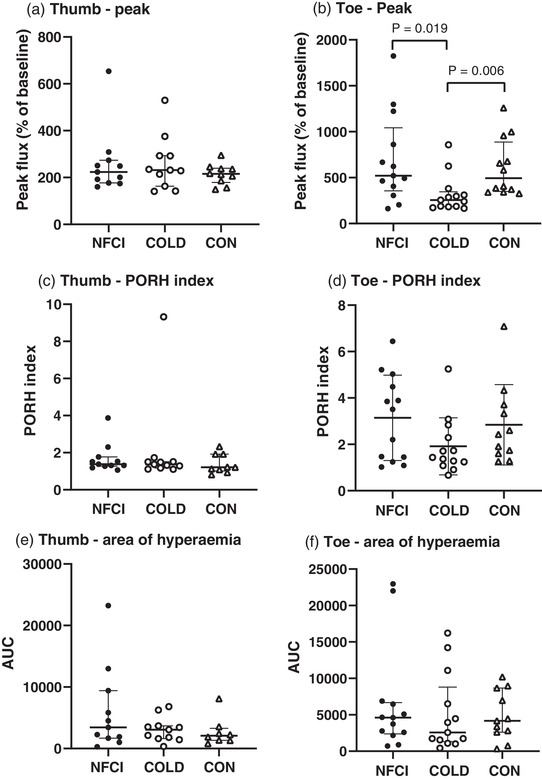
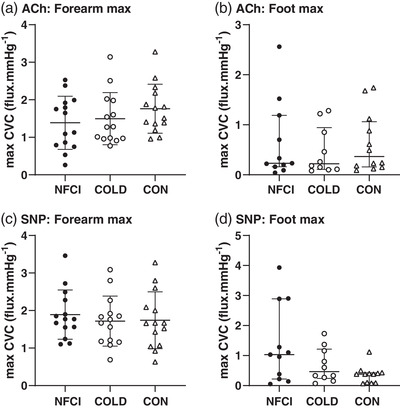
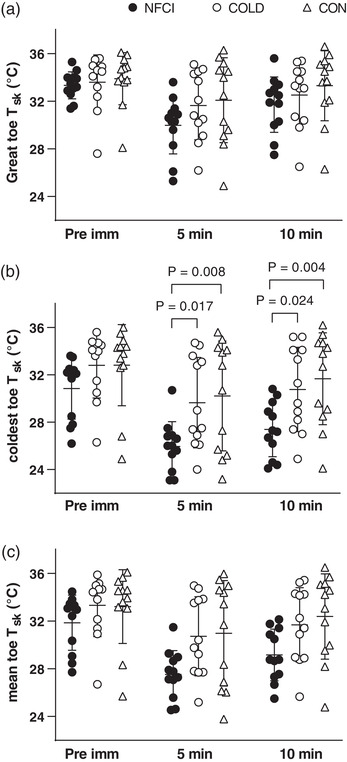
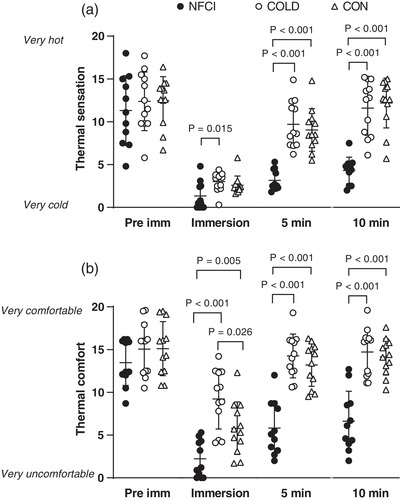
Abstract: The impact of non-freezing cold injury (NFCI) on peripheral vascular function was investigated. Individuals with NFCI (NFCI group) and closely matched controls with either similar (COLD group) or limited (CON group) previous cold exposure were compared (n = 16). Peripheral cutaneous vascular responses to deep inspiration (DI), occlusion (PORH), local cutaneous heating (LH) and iontophoresis of acetylcholine and sodium nitroprusside were investigated. The responses to a cold sensitivity test (CST) involving immersion of a foot in 15°C water for 2 min followed by spontaneous rewarming, and a foot cooling protocol (footplate cooled from 34°C to 15°C), were also examined. The vasoconstrictor response to DI was lower in NFCI compared to CON (toe: 73 (28)% vs. 91 (17)%; P = 0.003). The responses to PORH, LH and iontophoresis were not reduced compared to either COLD or CON. During the CST, toe skin temperature rewarmed more slowly in NFCI than COLD or CON (10 min: 27.4 (2.3)°C vs. 30.7 (3.7)°C and 31.7 (3.9)°C, P < 0.05, respectively); however, no differences were observed during the footplate cooling. NFCI were more cold-intolerant (P < 0.0001) and reported colder and more uncomfortable feet during the CST and footplate cooling than COLD and CON (P < 0.05). NFCI showed a decreased sensitivity to sympathetic vasoconstrictor activation than CON and greater cold sensitivity (CST) compared to COLD and CON. None of the other vascular function tests indicated endothelial dysfunction. However, NFCI perceived their extremities to be colder and more uncomfortable/painful than the controls.
Keywords: cold injury; pathophysiology; vascular.
© 2023 The Authors. Experimental Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Conflict of interest statement
None of the authors have any conflicts of interest.
Figures
Comment in
-
Non-freezing cold injury: A little-known big problem.Exp Physiol. 2023 Mar;108(3):329-330. doi: 10.1113/EP091139. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36807674 Free PMC article. No abstract available.
Similar articles
-
Peripheral sensory function in non-freezing cold injury patients and matched controls.Exp Physiol. 2023 Mar;108(3):438-447. doi: 10.1113/EP090720. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36807948 Free PMC article.
-
Plasma biomarkers of endothelial function, inflammation and oxidative stress in individuals with non-freezing cold injury.Exp Physiol. 2023 Mar;108(3):448-464. doi: 10.1113/EP090722. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36808666 Free PMC article.
-
Previous recreational cold exposure does not alter endothelial function or sensory thermal thresholds in the hands or feet.Exp Physiol. 2021 Jan;106(1):328-337. doi: 10.1113/EP088555. Epub 2020 Jun 5. Exp Physiol. 2021. PMID: 32394510
-
Nonfreezing Cold Injury (Trench Foot).Int J Environ Res Public Health. 2021 Oct 6;18(19):10482. doi: 10.3390/ijerph181910482. Int J Environ Res Public Health. 2021. PMID: 34639782 Free PMC article. Review.
-
[Non-freezing cold injury in soldiers].Harefuah. 2002 Dec;141(12):1050-4, 1090. Harefuah. 2002. PMID: 12534203 Review. Hebrew.
Cited by
-
Peripheral sensory function in non-freezing cold injury patients and matched controls.Exp Physiol. 2023 Mar;108(3):438-447. doi: 10.1113/EP090720. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36807948 Free PMC article.
-
Plasma biomarkers of endothelial function, inflammation and oxidative stress in individuals with non-freezing cold injury.Exp Physiol. 2023 Mar;108(3):448-464. doi: 10.1113/EP090722. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36808666 Free PMC article.
-
The effect of acute hot water immersion on cutaneous peripheral microvascular responses in males of White-European, Black-African and South-Asian descent.Temperature (Austin). 2025 Jan 24;12(2):149-165. doi: 10.1080/23328940.2025.2453959. eCollection 2025. Temperature (Austin). 2025. PMID: 40330612 Free PMC article.
-
Cold weather operations: Preventive strategies in a military context.Temperature (Austin). 2024 Oct 23;12(1):8-27. doi: 10.1080/23328940.2024.2408059. eCollection 2025. Temperature (Austin). 2024. PMID: 40041157 Free PMC article. Review.
-
Non-freezing cold injury: A little-known big problem.Exp Physiol. 2023 Mar;108(3):329-330. doi: 10.1113/EP091139. Epub 2023 Feb 20. Exp Physiol. 2023. PMID: 36807674 Free PMC article. No abstract available.
References
-
- ACSM . (2010). Cardiorespiratory fitness: Estimation from field and submaximal exercise tests. In Health‐related physical fitness assessment manual (3rd ed.) Wolters.
-
- Ahle, N. W. , Buroni, J. R. , Sharp, M. W. , & Hamlet, M. P. (1990). Infrared thermographic measurement of circulatory compromise in trenchfoot‐injured Argentine soldiers. Aviation, Space, and Environmental Medicine, 61, 247–250. - PubMed
-
- Arnstein, P. , Caudill, M. , Mandle, C. L. , Norris, A. , & Beasley, R. (1999). Self efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain, 80(3), 483–491. - PubMed
-
- Arvesen, A. , Rosen, L. , Eltvik, L. P. , Kroese, A. , & Stranden, E. (1994). Skin microcirculation in patients with sequelae from local cold injuries. International Journal of Microcirculation, Clinical and Experimental, 14(6), 335–342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources