

Epidural stimulation of the cervical spinal cord for post-stroke upper-limb paresis
- PMID: 36807682
- PMCID: PMC10291889
- DOI: 10.1038/s41591-022-02202-6
Epidural stimulation of the cervical spinal cord for post-stroke upper-limb paresis
Abstract
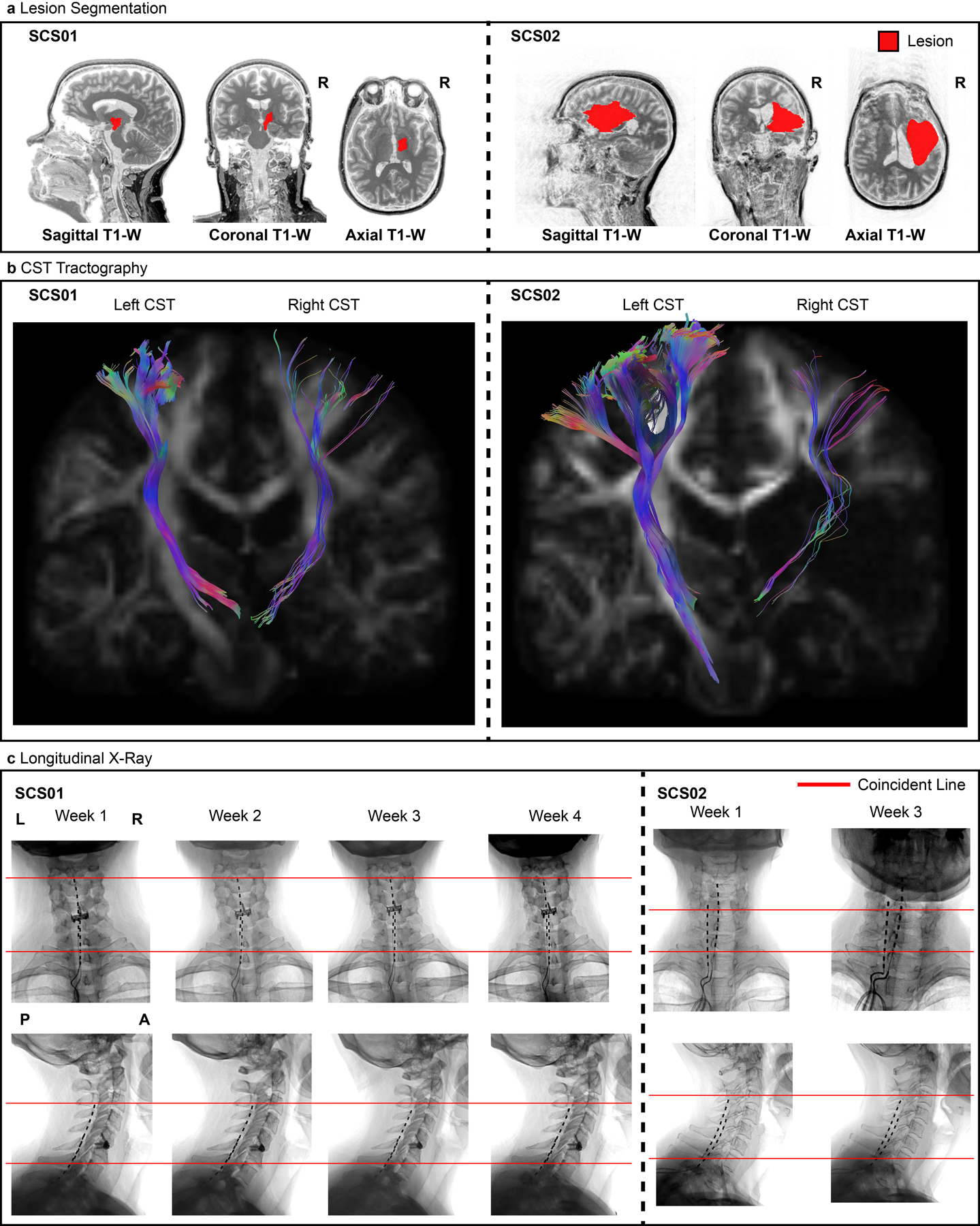
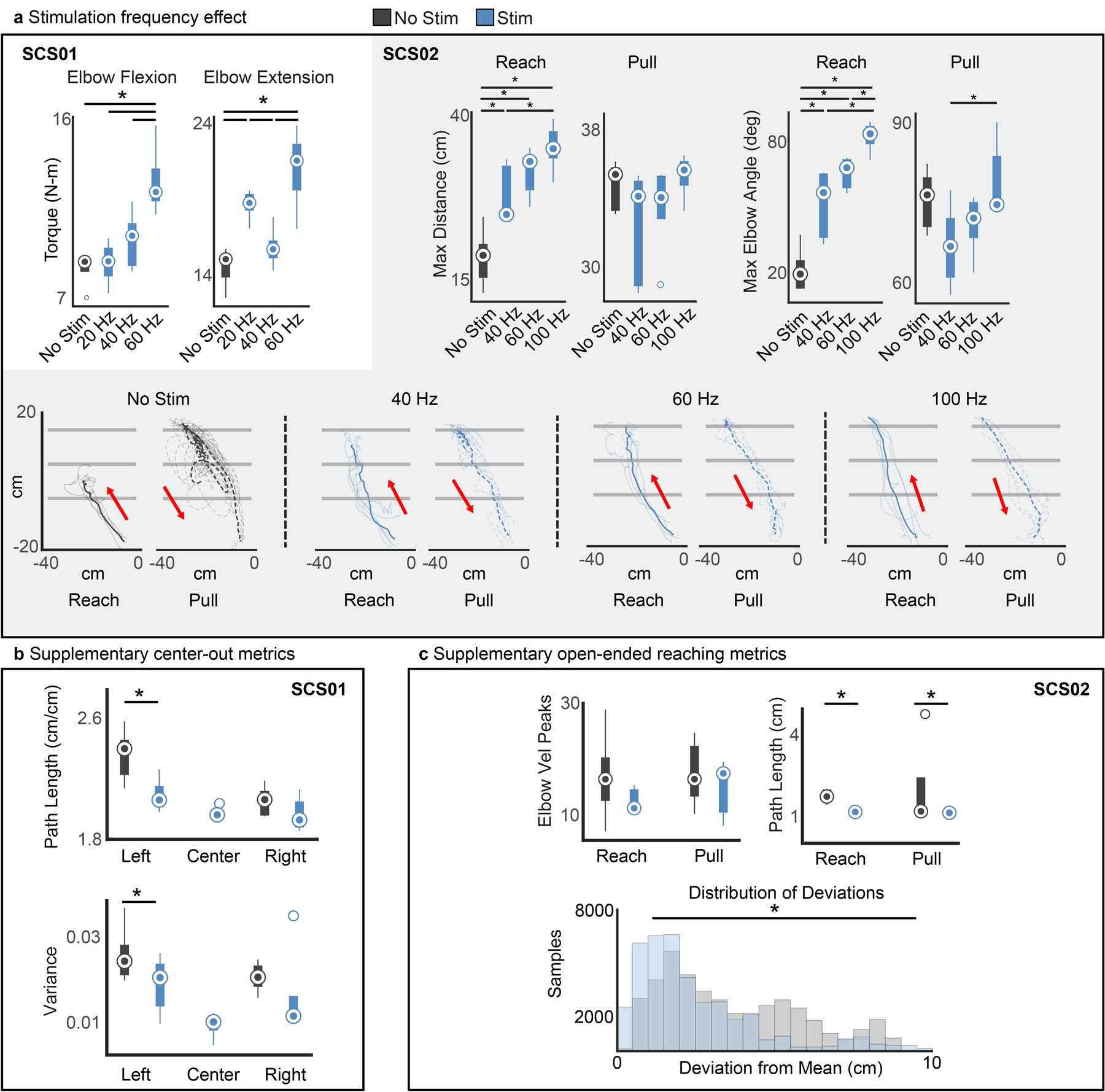
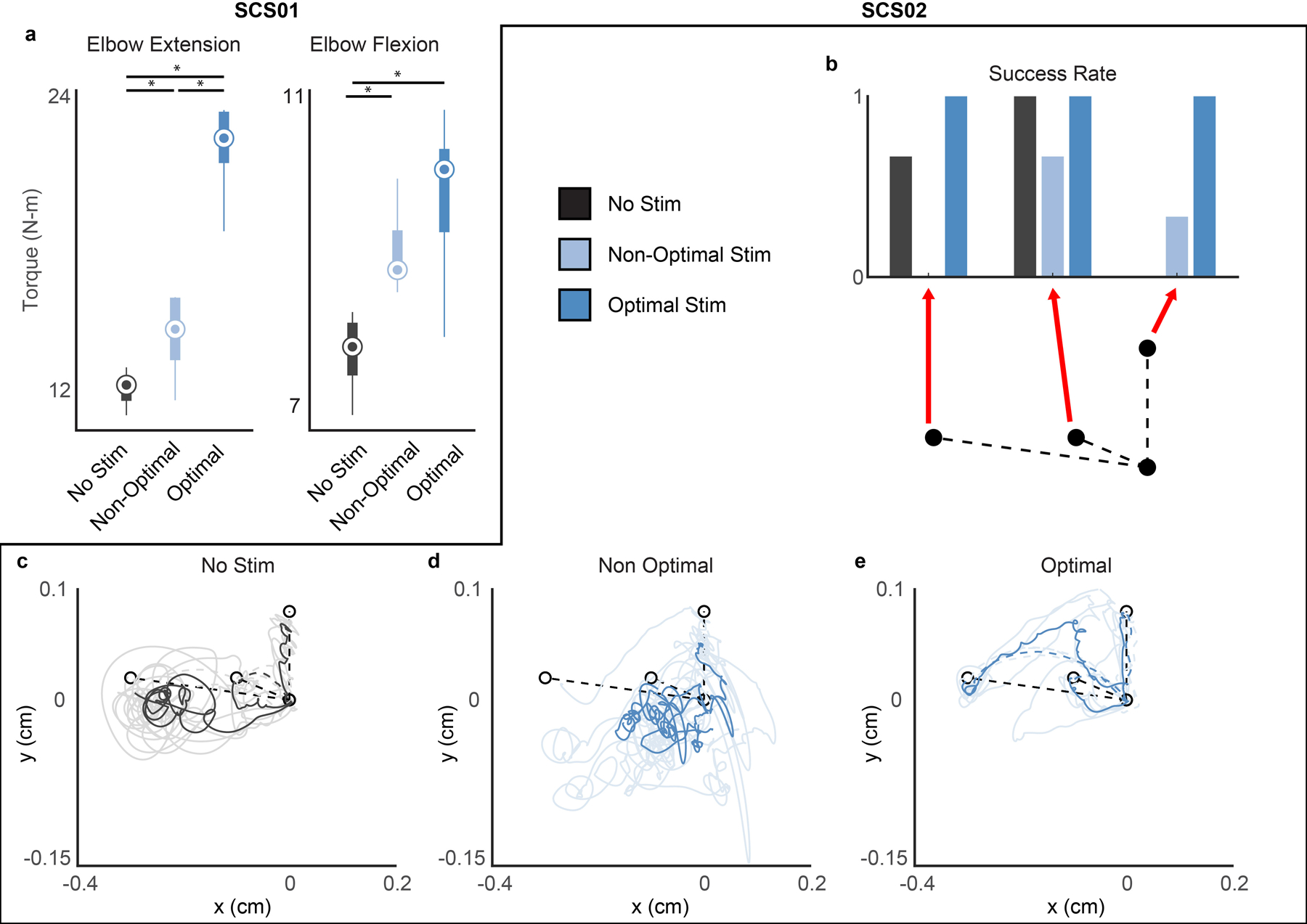
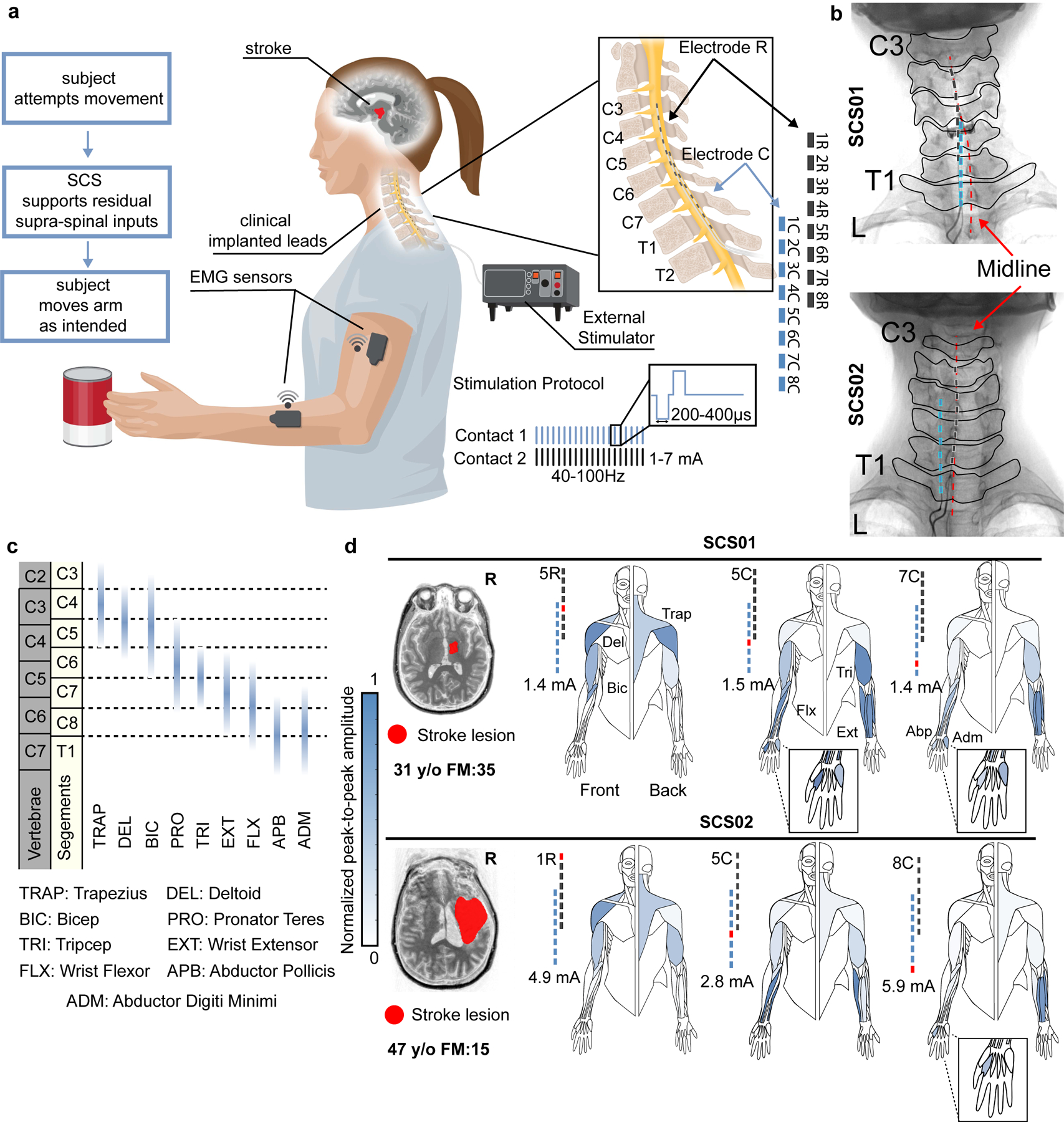
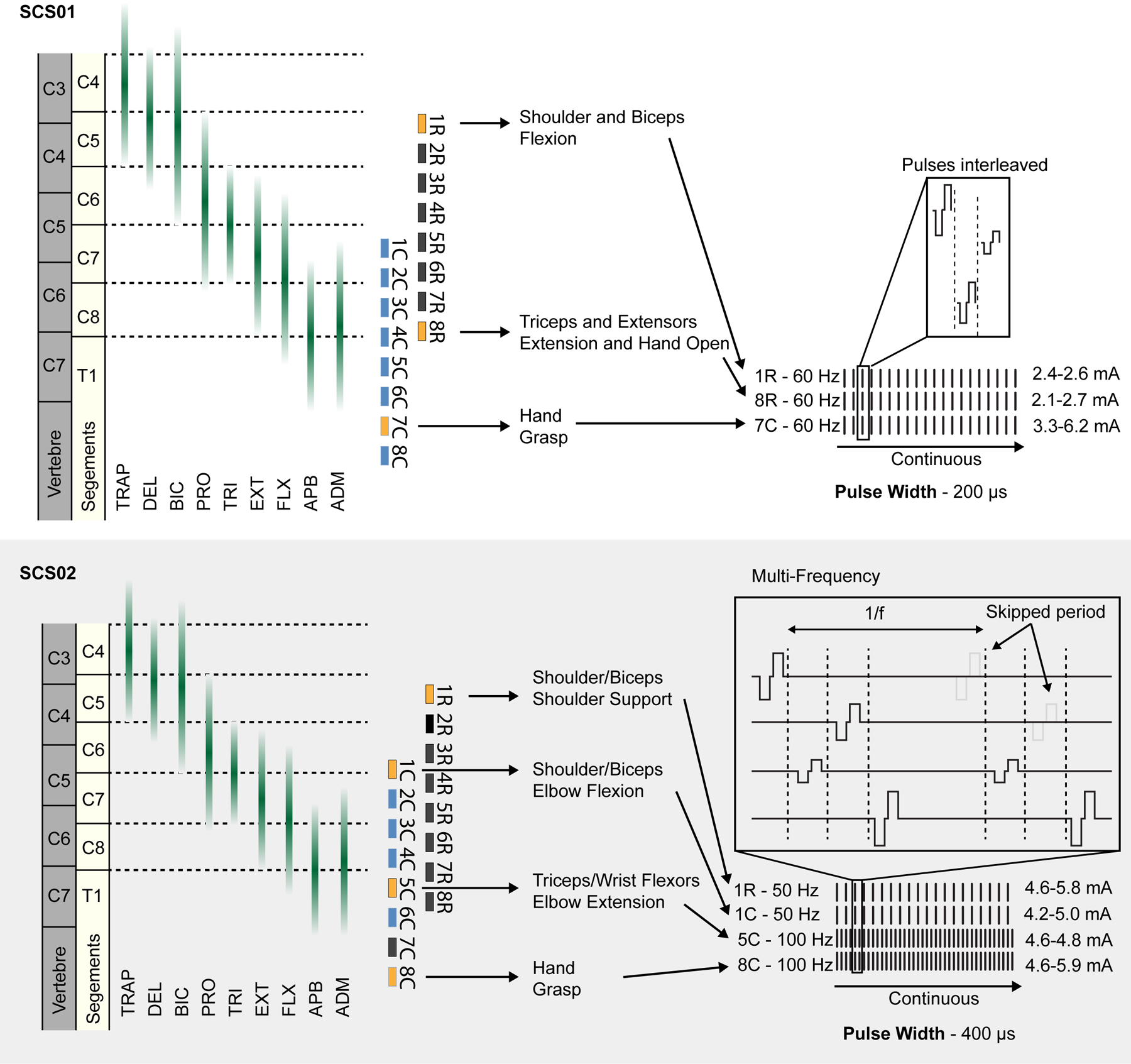
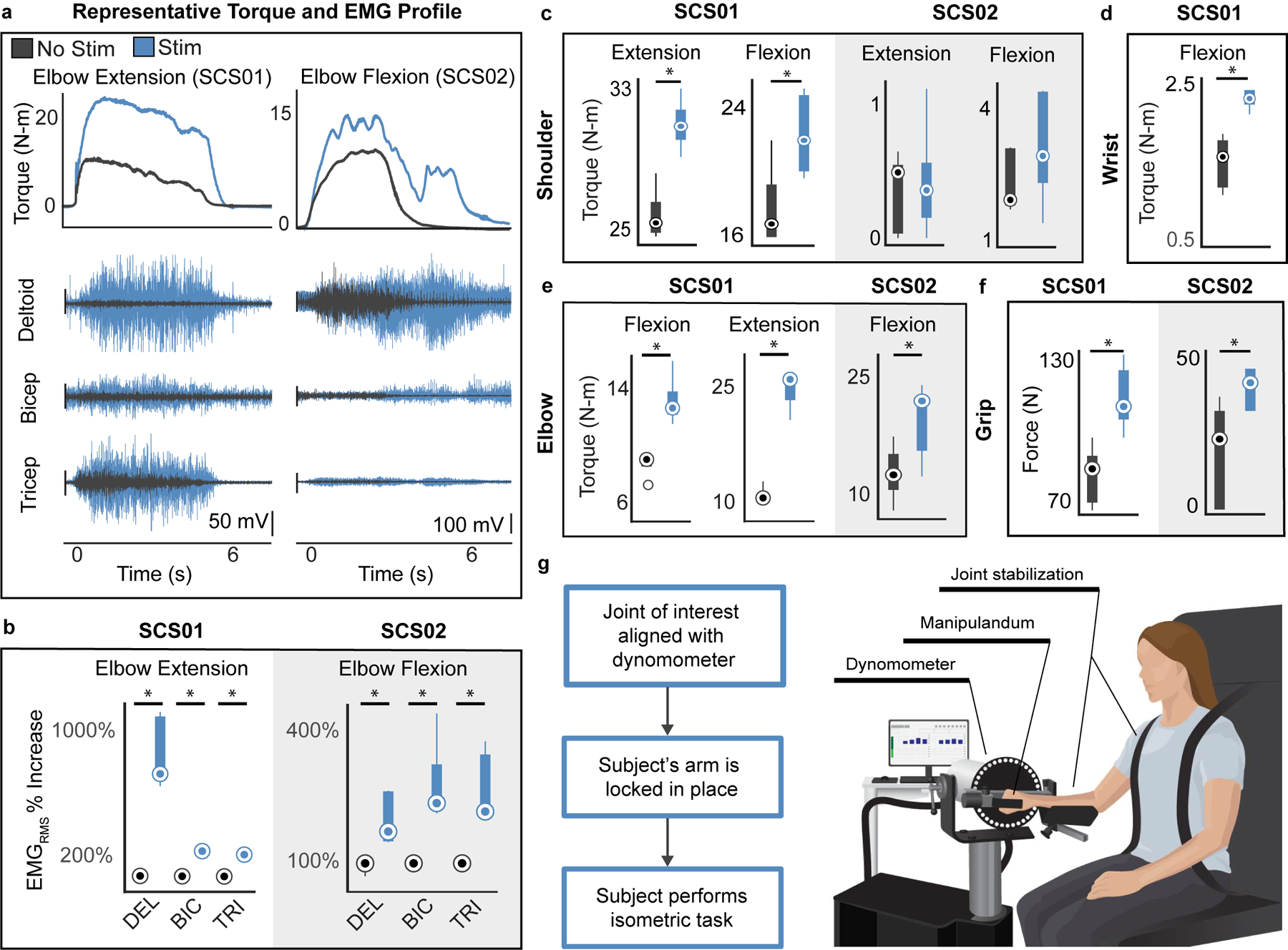
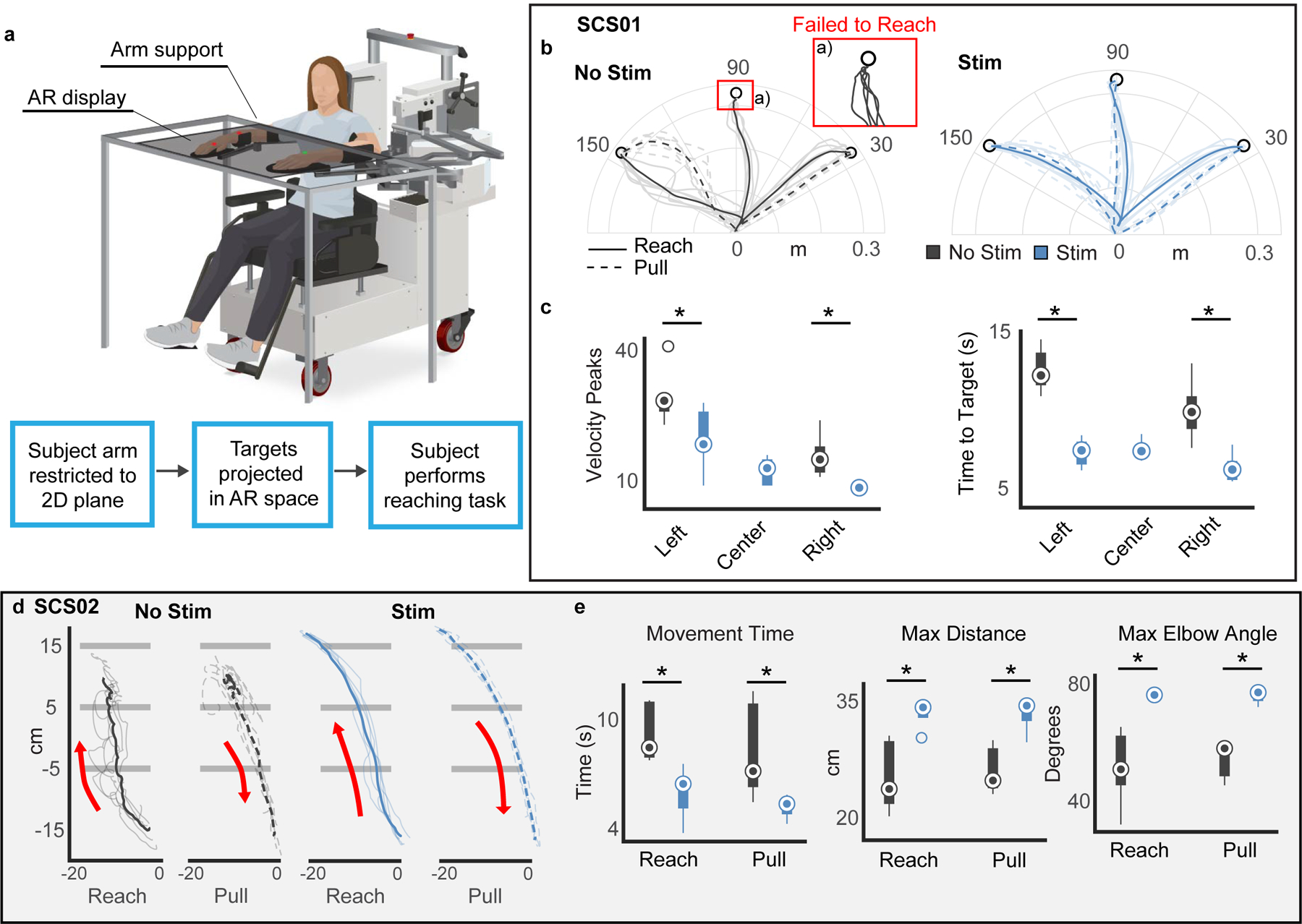
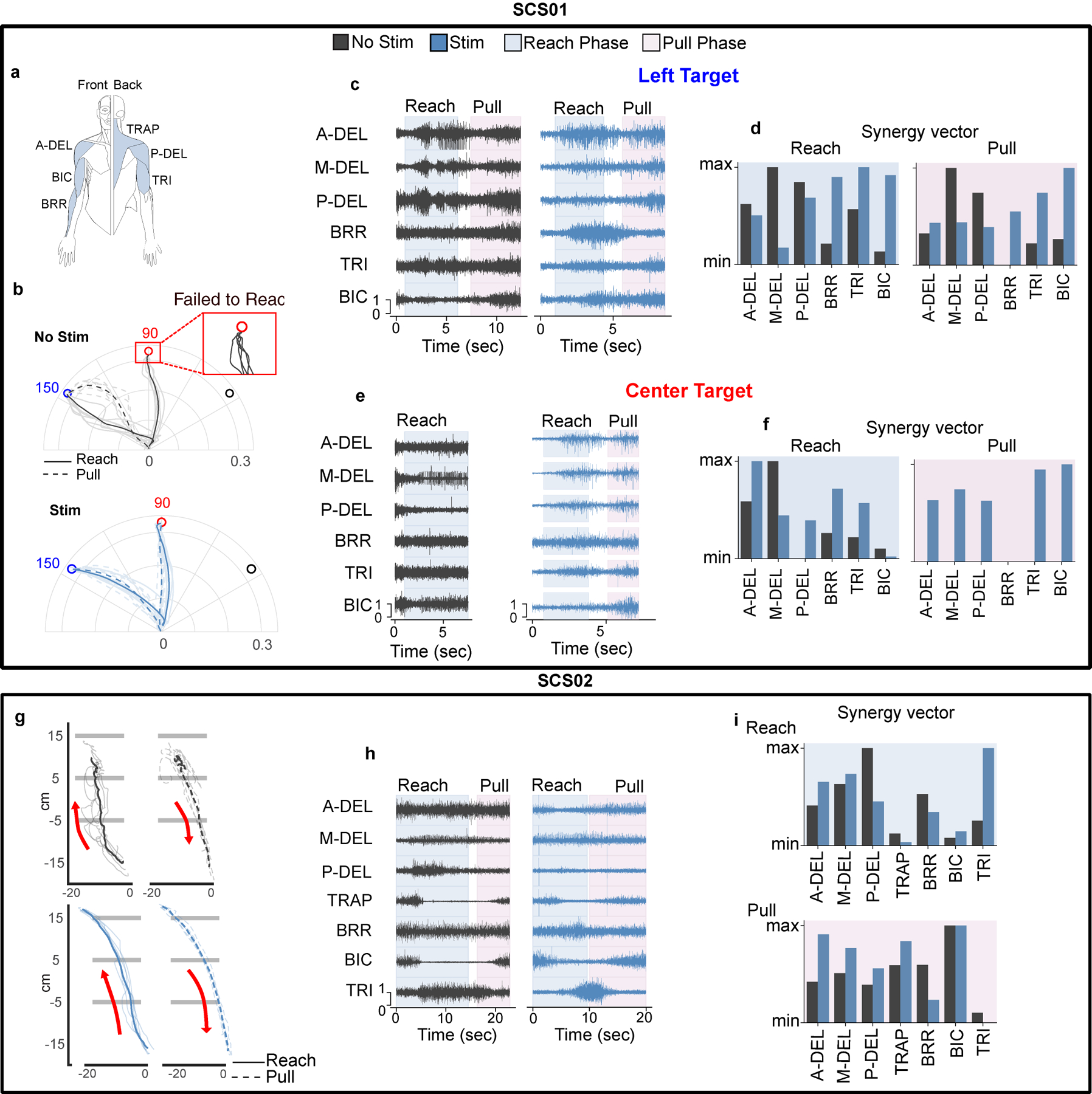
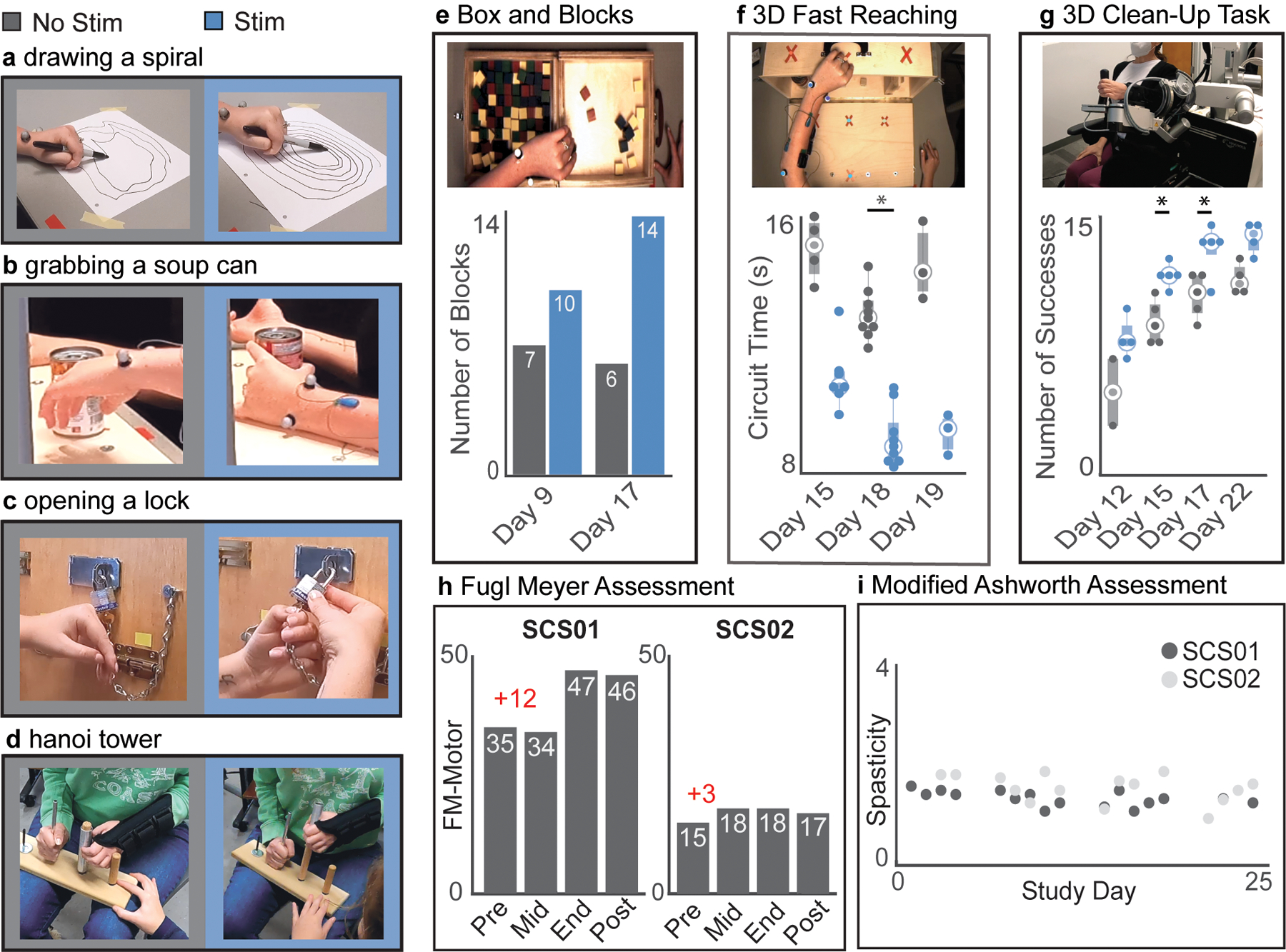
Cerebral strokes can disrupt descending commands from motor cortical areas to the spinal cord, which can result in permanent motor deficits of the arm and hand. However, below the lesion, the spinal circuits that control movement remain intact and could be targeted by neurotechnologies to restore movement. Here we report results from two participants in a first-in-human study using electrical stimulation of cervical spinal circuits to facilitate arm and hand motor control in chronic post-stroke hemiparesis ( NCT04512690 ). Participants were implanted for 29 d with two linear leads in the dorsolateral epidural space targeting spinal roots C3 to T1 to increase excitation of arm and hand motoneurons. We found that continuous stimulation through selected contacts improved strength (for example, grip force +40% SCS01; +108% SCS02), kinematics (for example, +30% to +40% speed) and functional movements, thereby enabling participants to perform movements that they could not perform without spinal cord stimulation. Both participants retained some of these improvements even without stimulation and no serious adverse events were reported. While we cannot conclusively evaluate safety and efficacy from two participants, our data provide promising, albeit preliminary, evidence that spinal cord stimulation could be an assistive as well as a restorative approach for upper-limb recovery after stroke.
© 2023. The Author(s), under exclusive licence to Springer Nature America, Inc.
Conflict of interest statement
COMPETING INTERESTS STATEMENT
MP, DW, MC and PG are founders and shareholders of Reach Neuro Inc. a company developing spinal cord stimulation technologies for stroke. EP has interest in Reach Neuro Inc due to personal relationship with MC. MP, DW, MC, PG, EP, ES, NV and EC are inventors on patents related to this work. All other authors declare no competing interests.
Figures
Comment in
-
Aspiring to restore arm and hand function after stroke.Lancet Neurol. 2023 Jun;22(6):464-465. doi: 10.1016/S1474-4422(23)00150-3. Lancet Neurol. 2023. PMID: 37210089 No abstract available.
References
-
- Lawrence ES et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 32, 1279–1284 (2001). - PubMed
-
- Virani SS et al. Heart Disease and Stroke Statistics—2021 Update: A Report From the American Heart Association. Circulation 143, (2021). - PubMed
-
- Krakauer JW & Carmichael ST Broken movement: the neurobiology of motor recovery after stroke. (MIT Press, 2017).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
