

In-depth virological and immunological characterization of HIV-1 cure after CCR5Δ32/Δ32 allogeneic hematopoietic stem cell transplantation
- PMID: 36807684
- PMCID: PMC10033413
- DOI: 10.1038/s41591-023-02213-x
In-depth virological and immunological characterization of HIV-1 cure after CCR5Δ32/Δ32 allogeneic hematopoietic stem cell transplantation
Abstract
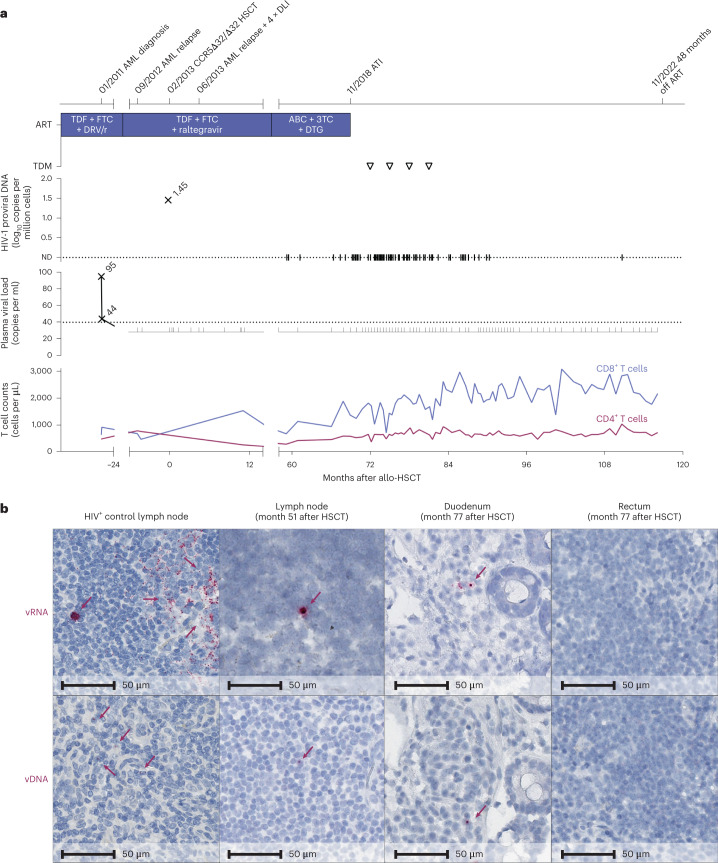
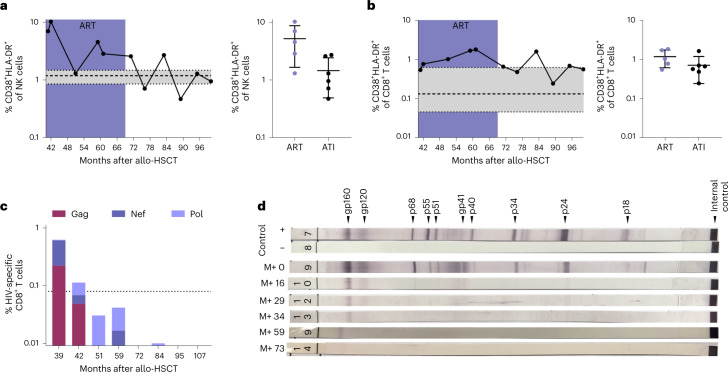
Despite scientific evidence originating from two patients published to date that CCR5Δ32/Δ32 hematopoietic stem cell transplantation (HSCT) can cure human immunodeficiency virus type 1 (HIV-1), the knowledge of immunological and virological correlates of cure is limited. Here we characterize a case of long-term HIV-1 remission of a 53-year-old male who was carefully monitored for more than 9 years after allogeneic CCR5Δ32/Δ32 HSCT performed for acute myeloid leukemia. Despite sporadic traces of HIV-1 DNA detected by droplet digital PCR and in situ hybridization assays in peripheral T cell subsets and tissue-derived samples, repeated ex vivo quantitative and in vivo outgrowth assays in humanized mice did not reveal replication-competent virus. Low levels of immune activation and waning HIV-1-specific humoral and cellular immune responses indicated a lack of ongoing antigen production. Four years after analytical treatment interruption, the absence of a viral rebound and the lack of immunological correlates of HIV-1 antigen persistence are strong evidence for HIV-1 cure after CCR5Δ32/Δ32 HSCT.
© 2023. The Author(s).
Conflict of interest statement
B.-E.O.J. received honoraria for presentations from Gilead, ViiV Healthcare, MSD and Janssen (unrelated to the submitted work) and served on advisory boards for ViiV Healthcare and Gilead (unrelated to the submitted work). N.L. received honoraria for presentations from Gilead, MSD, Abbvie and ViiV Healthcare and served on the advisory boards for ViiV Healthcare and Theratechnologies (all unrelated to the submitted work). C. Münk received a research grant from Gilead (unrelated to the submitted work). I.H. and J.H. are cofounders and shareholders of PROVIREX Genome Editing Therapies GmbH, a start-up company focusing on the excision of HIV-1 by genome editing (unrelated to this work). J.S.z.W. received lecture fees from Gilead (unrelated to the submitted work). A.M.J.W. received an unrestricted research grant from Gilead and did consultancy for Gilead, GlaxoSmithKline and ViiV Healthcare (unrelated to the submitted work). J.M.-P. received institutional grants and educational/consultancy fees from AbiVax, AstraZeneca, Gilead, Grifols, Janssen, Merck Sharp & Dohme and ViiV Healthcare (unrelated to the submitted work). The other authors declare no competing interests.
Figures





Comment in
-
Curating evidence for a cure of HIV-1 infection by hematopoietic stem cell transplantation.Med. 2023 May 12;4(5):285-287. doi: 10.1016/j.medj.2023.04.006. Med. 2023. PMID: 37178680 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
