

Association of anorexia/appetite loss with malnutrition and mortality in older populations: A systematic literature review
- PMID: 36807868
- PMCID: PMC10067499
- DOI: 10.1002/jcsm.13186
Association of anorexia/appetite loss with malnutrition and mortality in older populations: A systematic literature review
Abstract
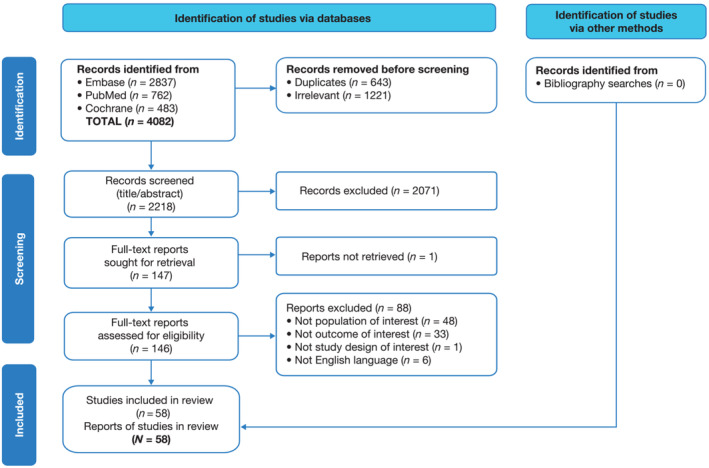
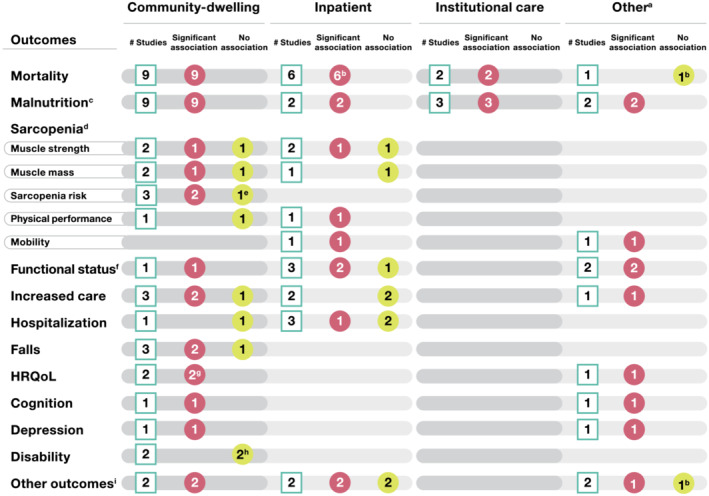
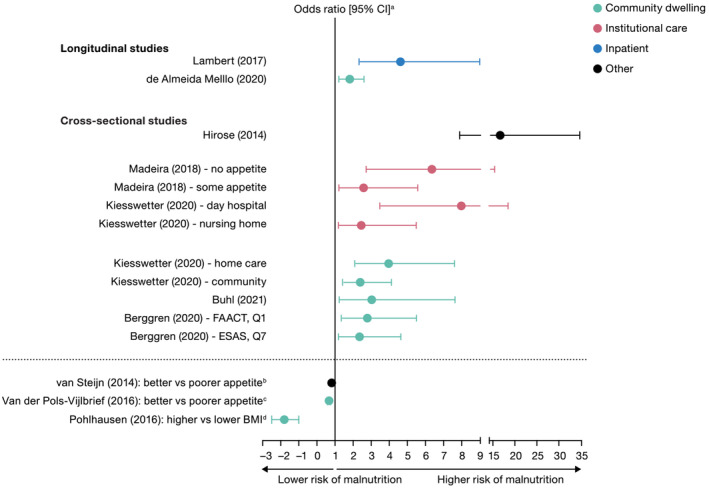
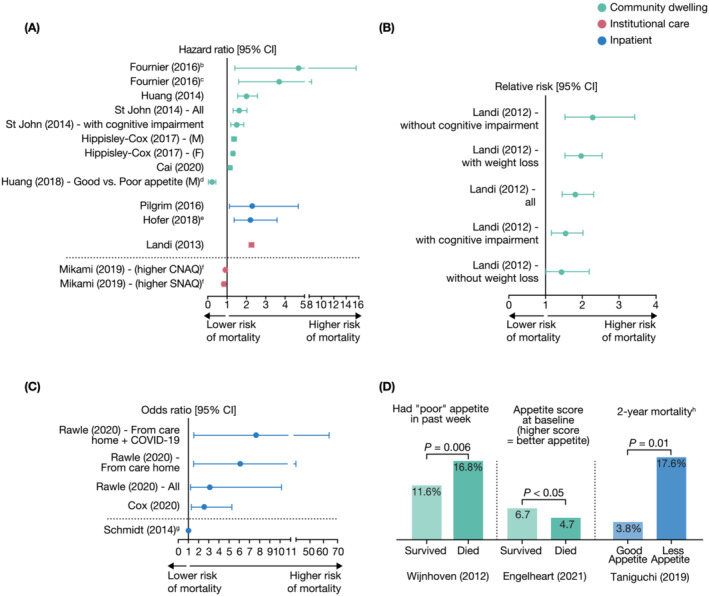
Anorexia/appetite loss in older subjects is frequently underrecognized in clinical practice, which may reflect deficient understanding of clinical sequelae. Therefore, we performed a systematic literature review to assess the morbidity and mortality burden of anorexia/appetite loss in older populations. Following PRISMA guidelines, searches were run (1 January 2011 to 31 July 2021) in PubMed, Embase® and Cochrane databases to identify English language studies of adults aged ≥ 65 years with anorexia/appetite loss. Two independent reviewers screened titles, abstracts and full text of identified records against pre-defined inclusion/exclusion criteria. Population demographics were extracted alongside risk of malnutrition, mortality and other outcomes of interest. Of 146 studies that underwent full-text review, 58 met eligibility criteria. Most studies were from Europe (n = 34; 58.6%) or Asia (n = 16; 27.6%), with few (n = 3; 5.2%) from the United States. Most were conducted in a community setting (n = 35; 60.3%), 12 (20.7%) were inpatient based (hospital/rehabilitation ward), 5 (8.6%) were in institutional care (nursing/care homes) and 7 (12.1%) were in other (mixed or outpatient) settings. One study reported results separately for community and institutional settings and is counted in both settings. Simplified Nutritional Appetite Questionnaire (SNAQ Simplified, n = 14) and subject-reported appetite questions (n = 11) were the most common methods used to assess anorexia/appetite loss, but substantial variability in assessment tools was observed across studies. The most commonly reported outcomes were malnutrition and mortality. Malnutrition was assessed in 15 studies, with all reporting a significantly higher risk of malnutrition in older individuals with anorexia/appetite loss (vs. without) regardless of country or healthcare setting (community n = 9, inpatient n = 2, institutional n = 3, other n = 2). Of 18 longitudinal studies that assessed mortality risk, 17 (94%) reported a significant association between anorexia/appetite loss and mortality regardless of either healthcare setting (community n = 9, inpatient n = 6, institutional n = 2) or method used to assess anorexia/appetite loss. This association between anorexia/appetite loss and mortality was observed in cohorts with cancer (as expected) but was also observed in older populations with a range of comorbid conditions other than cancer. Overall, our findings demonstrate that, among individuals aged ≥ 65 years, anorexia/appetite loss is associated with increased risk of malnutrition, mortality and other negative outcomes across community, care home and hospital settings. Such associations warrant efforts to improve and standardize screening, detection, assessment and management of anorexia/appetite loss in older adults.
Keywords: anorexia; appetite loss; malnutrition; mortality; prevalence; systematic literature review.
© 2023 Pfizer Inc and The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
Roger A. Fielding reports grants, personal fees and other from Axcella Health, other from Juvicell, other from Inside Tracker, grants and personal fees from Biophytis, personal fees from Amazentis, personal fees from Nestle and personal fees from Pfizer, outside the submitted work. Roger A. Fielding is also partially supported by the US Department of Agriculture (USDA), under Agreement No. 58‐8050‐9‐004 and by NIH Boston Claude D. Pepper Center (OAIC; 1P30AG031679). Any opinions, findings, conclusions or recommendations expressed in this publication are those of the authors and do not necessarily reflect the view of the USDA. Francesco Landi reports invited lectures for Abbott and Nutricia. Karen E. Smoyer is an employee of Curo, part of Envision Pharma group who were paid consultants to Pfizer in relation to this project. Lisa Tarasenko and John Groarke are employees of Pfizer and may hold stock or stock options.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
