

Cumulative 6-Year Risk of Screen-Detected Ductal Carcinoma In Situ by Screening Frequency
- PMID: 36808238
- PMCID: PMC9941892
- DOI: 10.1001/jamanetworkopen.2023.0166
Cumulative 6-Year Risk of Screen-Detected Ductal Carcinoma In Situ by Screening Frequency
Abstract
Importance: Detection of ductal carcinoma in situ (DCIS) by mammography screening is a controversial outcome with potential benefits and harms. The association of mammography screening interval and woman's risk factors with the likelihood of DCIS detection after multiple screening rounds is poorly understood.
Objective: To develop a 6-year risk prediction model for screen-detected DCIS according to mammography screening interval and women's risk factors.
Design, setting, and participants: This Breast Cancer Surveillance Consortium cohort study assessed women aged 40 to 74 years undergoing mammography screening (digital mammography or digital breast tomosynthesis) from January 1, 2005, to December 31, 2020, at breast imaging facilities within 6 geographically diverse registries of the consortium. Data were analyzed between February and June 2022.
Exposures: Screening interval (annual, biennial, or triennial), age, menopausal status, race and ethnicity, family history of breast cancer, benign breast biopsy history, breast density, body mass index, age at first birth, and false-positive mammography history.
Main outcomes and measures: Screen-detected DCIS defined as a DCIS diagnosis within 12 months after a positive screening mammography result, with no concurrent invasive disease.
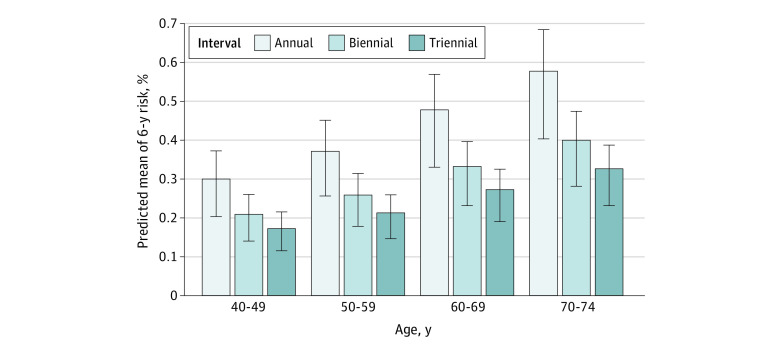
Results: A total of 916 931 women (median [IQR] age at baseline, 54 [46-62] years; 12% Asian, 9% Black, 5% Hispanic/Latina, 69% White, 2% other or multiple races, and 4% missing) met the eligibility criteria, with 3757 screen-detected DCIS diagnoses. Screening round-specific risk estimates from multivariable logistic regression were well calibrated (expected-observed ratio, 1.00; 95% CI, 0.97-1.03) with a cross-validated area under the receiver operating characteristic curve of 0.639 (95% CI, 0.630-0.648). Cumulative 6-year risk of screen-detected DCIS estimated from screening round-specific risk estimates, accounting for competing risks of death and invasive cancer, varied widely by all included risk factors. Cumulative 6-year screen-detected DCIS risk increased with age and shorter screening interval. Among women aged 40 to 49 years, the mean 6-year screen-detected DCIS risk was 0.30% (IQR, 0.21%-0.37%) for annual screening, 0.21% (IQR, 0.14%-0.26%) for biennial screening, and 0.17% (IQR, 0.12%-0.22%) for triennial screening. Among women aged 70 to 74 years, the mean cumulative risks were 0.58% (IQR, 0.41%-0.69%) after 6 annual screens, 0.40% (IQR, 0.28%-0.48%) for 3 biennial screens, and 0.33% (IQR, 0.23%-0.39%) after 2 triennial screens.
Conclusions and relevance: In this cohort study, 6-year screen-detected DCIS risk was higher with annual screening compared with biennial or triennial screening intervals. Estimates from the prediction model, along with risk estimates of other screening benefits and harms, could help inform policy makers' discussions of screening strategies.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
