

Optimal clinical protocols for total-body 18F-FDG PET/CT examination under different activity administration plans
- PMID: 36808378
- PMCID: PMC9938848
- DOI: 10.1186/s40658-023-00533-y
Optimal clinical protocols for total-body 18F-FDG PET/CT examination under different activity administration plans
Abstract
Background: Highly sensitive digital total-body PET/CT scanners (uEXPLORER) have great potential for clinical applications and fundamental research. Given their increasing sensitivity, low-dose scanning or snapshot imaging is now possible in clinics. However, a standardized total-body 18F-FDG PET/CT protocol is still lacking. Establishing a standard clinical protocol for total-body 18F-FDG PET/CT examination under different activity administration plans can help provide a theoretical reference for nuclear radiologists.
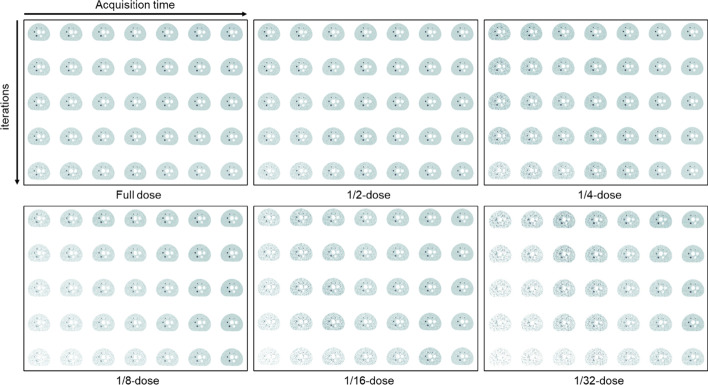
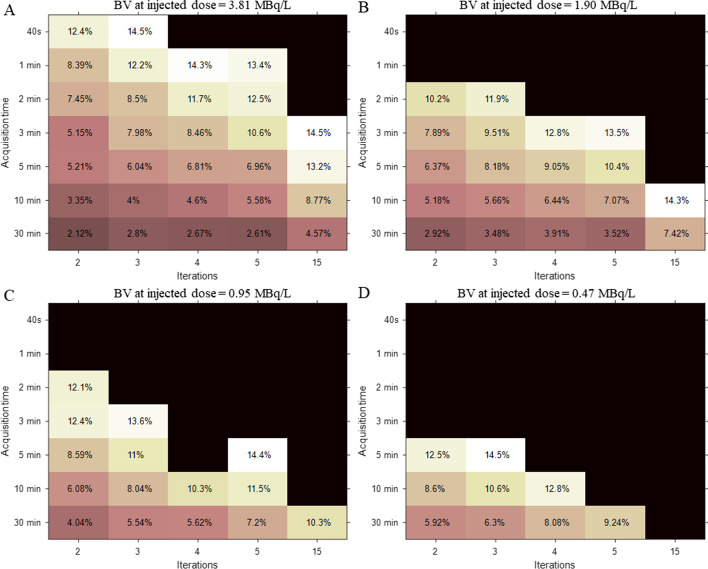
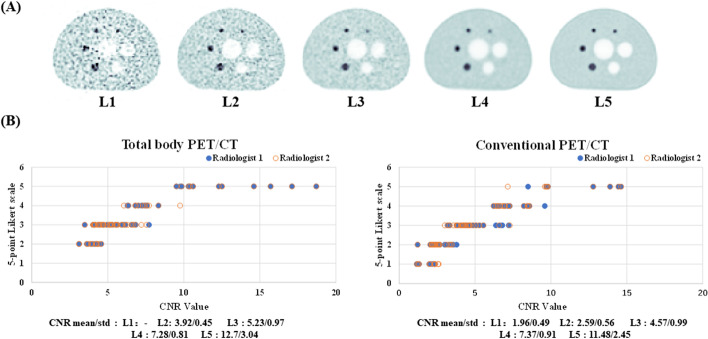
Methods: The NEMA image quality (IQ) phantom was used to evaluate the biases of various total-body 18F-FDG PET/CT protocols related to the administered activity, scan duration, and iterations. Several objective metrics, including contrast recovery (CR), background variability (BV), and contrast-to-noise ratio (CNR), were measured from different protocols. In line with the European Association of Nuclear Medicine Research Ltd. (EARL) guidelines, optimized protocols were suggested and evaluated for total-body 18F-FDG PET/CT imaging for three different injected activities.
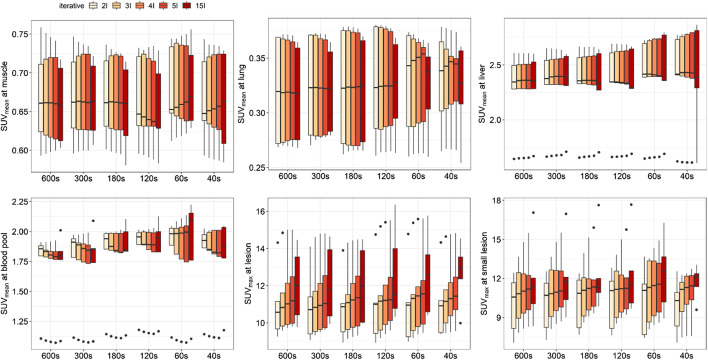
Results: Our NEMA IQ phantom evaluation resulted in total-body PET/CT images with excellent contrast and low noise, suggesting great potential for reducing administered activity or shortening the scan duration. Different to the iteration number, prolonging the scan duration was the first choice for achieving higher image quality regardless of the activity administered. In light of image quality, tolerance of oncological patients, and the risk of ionizing radiation damage, the 3-min acquisition and 2-iteration (CNR = 7.54), 10-min acquisition and 3-iteration (CNR = 7.01), and 10-min acquisition and 2-iteration (CNR = 5.49) protocols were recommended for full-dose (3.70 MBq/kg), half-dose (1.95 MBq/kg), and quarter-dose (0.98 MBq/kg) activity injection schemes, respectively. Those protocols were applied in clinical practices, and no significant differences were observed for the SUVmax of large/small lesions or the SUVmean of different healthy organs/tissues.
Conclusion: These findings support that digital total-body PET/CT scanners can generate PET images with a high CNR and low-noise background, even with a short acquisition time and low administered activity. The proposed protocols for different administered activities were determined to be valid for clinical examination and can maximize the value of this imaging type.
Keywords: 18F-FDG; Fast scanning; Low-dose; Protocol optimization; Total-body PET/CT.
© 2023. The Author(s).
Conflict of interest statement
Jiatai Feng and Jingyi Wang are employees of United Imaging Healthcare. Wanbang Xu works at the Department of Traditional Chinese Medicine in Guangdong Institute for Drug Control. The other authors working at Nanfang PET Center in Nanfang Hospital Southern Medical University have full control of the data and Nanfang hospital do not have any revenue sharing with other two Institutes. No other potential conflicts of interest relevant to this article exist including employment, royalties, stock options, or patients.
Figures


References
Grants and funding
- 11205081/the National Natural Science Foundation of China
- 2014A020212175/Science and Technology Planning Project of Guangdong Province
- 2020L002/President Foundation Project of Nanfang Hospital, Southern Medical University
- 2021C017/President Foundation Project of Nanfang Hospital, Southern Medical University
LinkOut - more resources
Full Text Sources
