

Hybrid laparoscopic versus fully robot-assisted minimally invasive esophagectomy: an international propensity-score matched analysis of perioperative outcome
- PMID: 36808472
- PMCID: PMC10234920
- DOI: 10.1007/s00464-023-09911-0
Hybrid laparoscopic versus fully robot-assisted minimally invasive esophagectomy: an international propensity-score matched analysis of perioperative outcome
Abstract
Background: Currently, little is known regarding the optimal technique for the abdominal phase of RAMIE. The aim of this study was to investigate the outcome of robot-assisted minimally invasive esophagectomy (RAMIE) in both the abdominal and thoracic phase (full RAMIE) compared to laparoscopy during the abdominal phase (hybrid laparoscopic RAMIE).
Methods: This retrospective propensity-score matched analysis of the International Upper Gastrointestinal International Robotic Association (UGIRA) database included 807 RAMIE procedures with intrathoracic anastomosis between 2017 and 2021 from 23 centers.
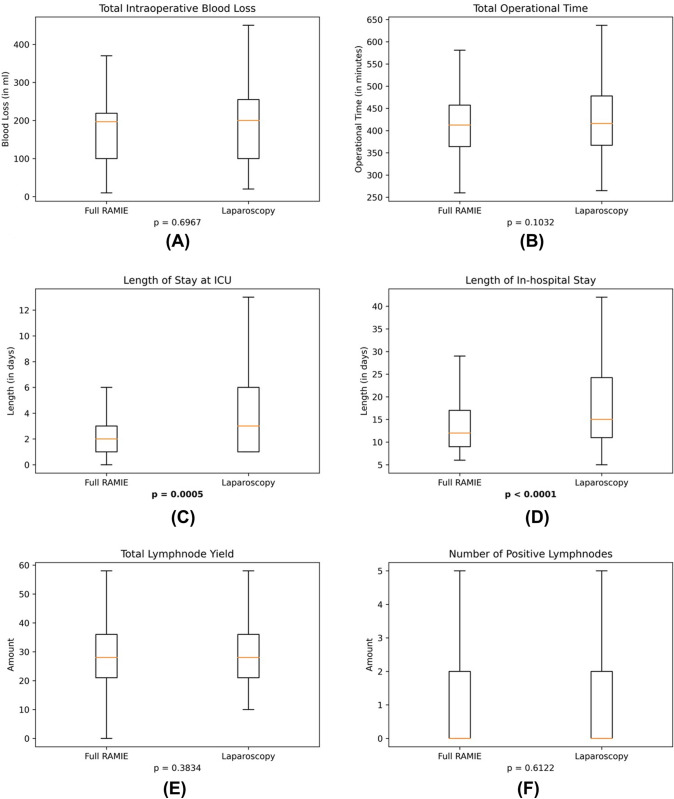
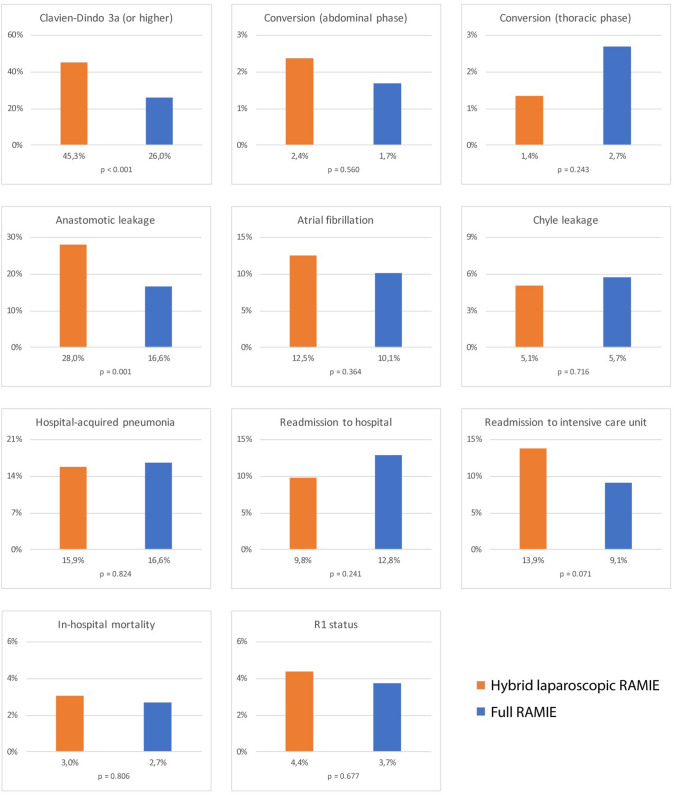
Results: After propensity-score matching, 296 hybrid laparoscopic RAMIE patients were compared to 296 full RAMIE patients. Both groups were equal regarding intraoperative blood loss (median 200 ml versus 197 ml, p = 0.6967), operational time (mean 430.3 min versus 417.7 min, p = 0.1032), conversion rate during abdominal phase (2.4% versus 1.7%, p = 0.560), radical resection (R0) rate (95.6% versus 96.3%, p = 0.8526) and total lymph node yield (mean 30.4 versus 29.5, p = 0.3834). The hybrid laparoscopic RAMIE group showed higher rates of anastomotic leakage (28.0% versus 16.6%, p = 0.001) and Clavien Dindo grade 3a or higher (45.3% versus 26.0%, p < 0.001). The length of stay on intensive care unit (median 3 days versus 2 days, p = 0.0005) and in-hospital (median 15 days versus 12 days, p < 0.0001) were longer for the hybrid laparoscopic RAMIE group.
Conclusions: Hybrid laparoscopic RAMIE and full RAMIE were oncologically equivalent with a potential decrease of postoperative complications and shorter (intensive care) stay after full RAMIE.
Keywords: Complications; Hybrid laparoscopic approach; Perioperative outcome; Propensity-score matching; RAMIE; Robot-assisted minimally invasive esophagectomy.
© 2023. The Author(s).
Conflict of interest statement
Drs. Richard van Hillegersberg, Peter P Grimminger and Jelle P Ruurda are consultants for Medtronic and proctors for Intuitive Surgical. Drs. Daniel Perez and Marc J van Det are proctors for Intuitive Surgical. Dr. Mark I van Berge Henegouwen is consultant for Mylan, Johnson & Johnson, Alesi Surgical, B. Braun, Medtronic, and received unrestricted research grants from Stryker (all fees paid to institution). Dr. Yin-Kai Chao is consultant for Intuitive Surgical and received a research grant from Intuitive Surgical. Drs. Christiane J Bruns and Hans F Fuchs are both consultants for Medtronic and received an educational grant from Intuitive Surgical. Drs. Jin-On Jung, Eline M de Groot, B Feike Kingma, Benjamin Babic, Jens P Hölzen, Jan W Haveman, Philippe Rouanet, Frank Benedix, Hecheng Li, Inderpal Sarkaria, Gijs I van Boxel, Philip Chiu, Jan-Hendrik Egberts, Rubens Sallum, Arul Immanuel, Paul Turner, Donald E Low, Michal Hubka, Paolo Strignano, Matthias Biebl and M Asif Chaudry have no conflicts of interest or financial ties to disclose.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
