

Coronavirus Disease 2019 Convalescent Plasma Outpatient Therapy to Prevent Outpatient Hospitalization: A Meta-Analysis of Individual Participant Data From 5 Randomized Trials
- PMID: 36809473
- PMCID: PMC10273382
- DOI: 10.1093/cid/ciad088
Coronavirus Disease 2019 Convalescent Plasma Outpatient Therapy to Prevent Outpatient Hospitalization: A Meta-Analysis of Individual Participant Data From 5 Randomized Trials
Abstract
Background: Outpatient monoclonal antibodies are no longer effective and antiviral treatments for coronavirus disease 2019 (COVID-19) disease remain largely unavailable in many countries worldwide. Although treatment with COVID-19 convalescent plasma (CCP) is promising, clinical trials among outpatients have shown mixed results.
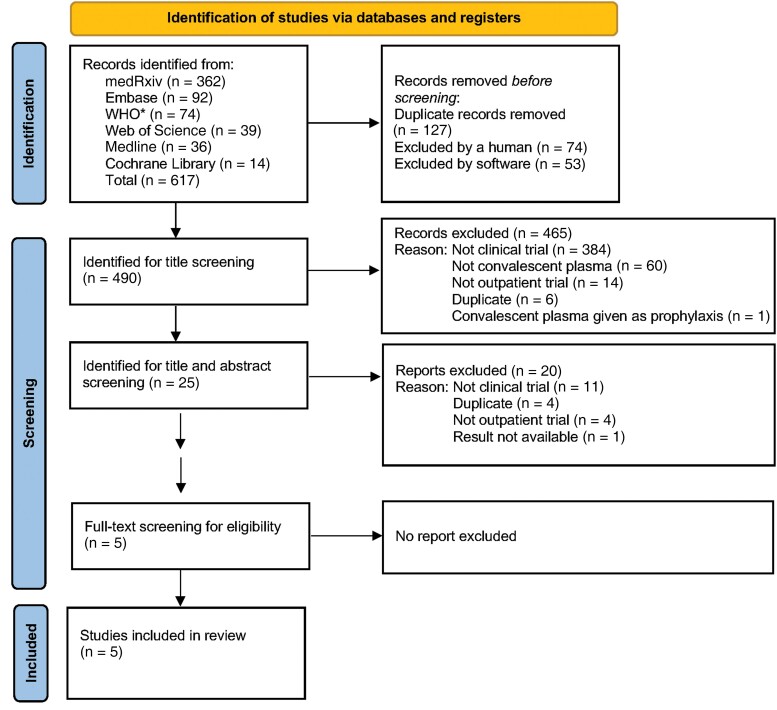
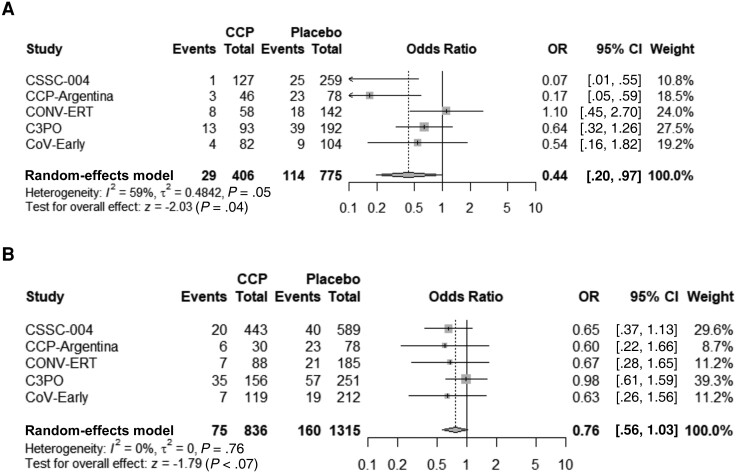
Methods: We conducted an individual participant data meta-analysis from outpatient trials to assess the overall risk reduction for all-cause hospitalizations by day 28 in transfused participants. Relevant trials were identified by searching Medline, Embase, medRxiv, World Health Organization COVID-19 Research Database, Cochrane Library, and Web of Science from January 2020 to September 2022.
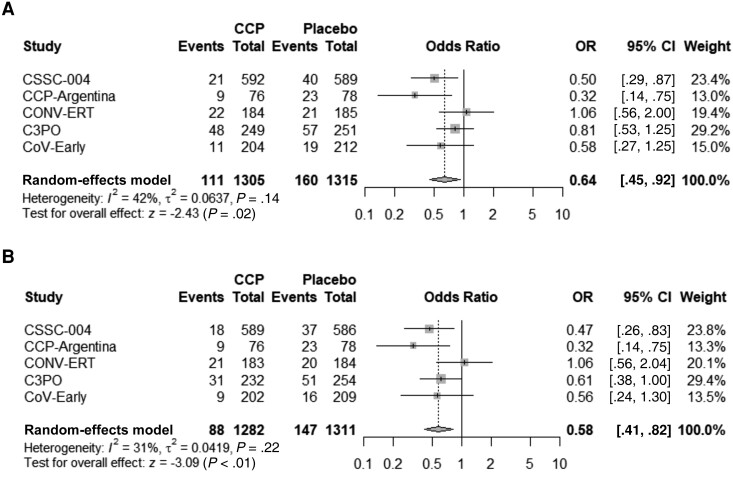
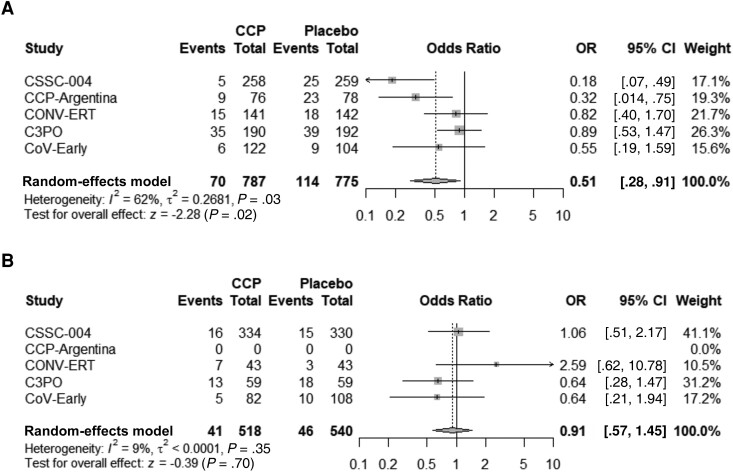
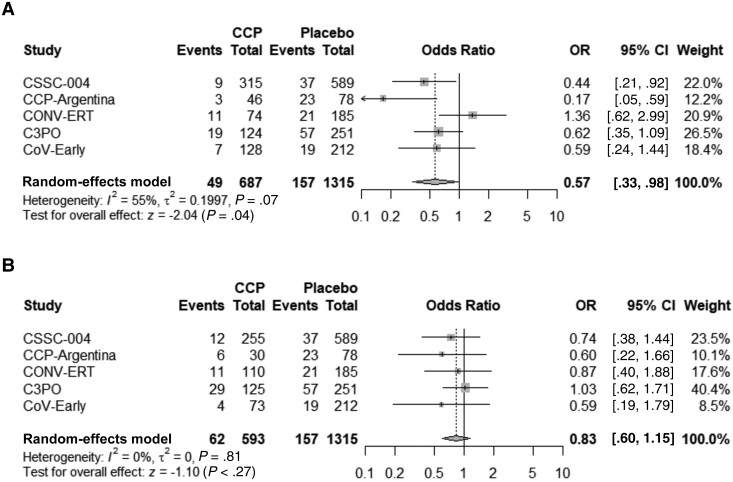
Results: Five included studies from 4 countries enrolled and transfused 2620 adult patients. Comorbidities were present in 1795 (69%). The virus neutralizing antibody dilutional titer levels ranged from 8 to 14 580 in diverse assays. One hundred sixty of 1315 (12.2%) control patients were hospitalized, versus 111 of 1305 (8.5%) CCP-treated patients, yielding a 3.7% (95% confidence interval [CI], 1.3%-6.0%; P = .001) absolute risk reduction and 30.1% relative risk reduction for all-cause hospitalization. The hospitalization reduction was greatest in those with both early transfusion and high titer with a 7.6% absolute risk reduction (95% CI, 4.0%-11.1%; P = .0001) accompanied by at 51.4% relative risk reduction. No significant reduction in hospitalization was seen with treatment >5 days after symptom onset or in those receiving CCP with antibody titers below the median titer.
Conclusions: Among outpatients with COVID-19, treatment with CCP reduced the rate of all-cause hospitalization and may be most effective when given within 5 days of symptom onset and when antibody titer is higher.
Keywords: COVID-19; COVID-19 convalescent plasma; SARS-CoV-2; hospitalization; therapy.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. R. L. has received fees from Pfizer for serving as subinvestigator of a COVID vaccine trial. F. P. has received fees from Pfizer for serving as a principal investigator for a COVID vaccine trial. D. J. S. is a founder and board member of AliquantumRx with stock options; Hemex Health malaria diagnostics consulting; royalties for malaria diagnostic test control standards from Alere (Binax Inc/D/B/A Inverness Medical); consulting fees for legal malaria case from Mabrey Firm (2019); the following grants or contracts: NIH/NIAID R01AI150763, NIH R21TR001737, NIH R01AI111962, DOD TB210115 (CDMRP Tick-Borne Disease Research Program); the following patents: USP 9642865 (issued 9 May 2017, New angiogenesis inhibitors), USP 7270948 (issued 18 September 2007, Detection of malaria parasites by laser desorption mass spectrometry), Salts and polymorphs of cethromycin for the treatment of disease (pending, application 20210163522), and Macrolide compounds and their use in liver stage malaria and related disease (pending, application PCT/US2015/046665); and participation on 2018 NIAID Safety Monitoring Committee/Independent Safety Monitor Intramural, all outside the submitted work. B. J. A. R. reports advisory board membership for Roche and AstraZeneca on a COVID-19 therapy; membership on a data and safety monitoring board (DSMB) for Exevir; consulting fees from Roche and AstraZeneca; grants or contracts and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events from Gilead Sciences; and support for attending meetings and/or travel from Pfizer. J. J. Z. reports consulting fees from City of Hope; cell therapy consultant; participation on DSMB for the PACER trial; DSMB for the Tolerant trial; and advisory boards for Sanofi and Sobi. L. J. D. reports the following grants or contracts: 75A50120C00094 (BARDA), Collection, testing, and provision of COVID-19 convalescent plasma for NHLBI/NIH (C3PO) through America's Blood Centers; US Veterans Health Administration, Pittsburgh (contract number 36C24E20D0027, VA CURES-1); and Vanderbilt University (Collection, testing, and provision of COVID-19 convalescent plasma for Association of Convalescent Plasma Treatment with Mortality and Clinical Trajectory in Patients Hospitalized with COVID-19 in the Community Setting). B. P. reports the following grants or contracts: COVID Trials, Incyte, Parexel, Novartis Pharmaceuticals, Partner Therapeutics, Fulcrum Therapeutics (to University Health Science Center), and Pulmonary Hypertension Trials, United Therapeutics, GlaxoSmithKline, Insmed, Merck Sharp & Dohme (to University of Texas Health Center). C. W. C. reports consulting honorarium for participation on NHLBI ACTIV4 CONNECTS Steering Committee. I. E. reports support for attending meetings and/or travel for 50 Congreso Argentino de Medicina Respiratoria 2022, Abstract Scholarship, American Thoracic Society, International Conference in Philadelphia, 2020 Assembly on Pediatrics. G. P. M. reports grants or contracts from Pfizer, Moderna, Medicago, and Merck for clinical research (as principal investigator), and payment for presentations from Moderna. D. O. reports consulting fees paid to author from the Fight Infectious Diseases Foundation and the Infectious Diseases Department, Hospital Universitari Germans Trias i Pujol. B. R. M. reports the following grants or contracts: NIH/NIAID R01AI150763, NIH R21TR001737, NIH R01AI111962, and DOD TB210115 (CDMRP Tick-Borne Disease Research Program). D. W. reports payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events from AstraZeneca, and support for attending meetings and/or travel from Laboratorios Raffo. C. R. reports grants or contracts from Gilead Sciences, ViiV Healthcare, Janssen-Cilag, AIDSfonds, and Health∼Holland; participation on a DSMB or advisory board as well as support for attending meetings and/or travel from Gilead Sciences and ViiV Healthcare; and gifts for the #awarehivukraine foundation. M. A. H. reports grants or contracts from Gilead, Insmed, and AN2 Therapeutics, as well as participation on the AIDS Clinical Trials Group Tuberculosis Transformative Science Group Study Monitoring Committee. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Update of
-
COVID-19 Convalescent Plasma Outpatient Therapy to Prevent Outpatient Hospitalization: A Meta-analysis of Individual Participant Data From Five Randomized Trials.medRxiv [Preprint]. 2022 Dec 18:2022.12.16.22283585. doi: 10.1101/2022.12.16.22283585. medRxiv. 2022. Update in: Clin Infect Dis. 2023 Jun 16;76(12):2077-2086. doi: 10.1093/cid/ciad088. PMID: 36561181 Free PMC article. Updated. Preprint.
Comment in
-
Coronavirus Disease 2019 Convalescent Plasma Reaches the Slope of Enlightenment in the Gartner Hype Cycle.Clin Infect Dis. 2023 Jun 16;76(12):2087-2089. doi: 10.1093/cid/ciad092. Clin Infect Dis. 2023. PMID: 36809542 No abstract available.
References
-
- Newland M, Durham D, Asher J, et al. Improving pandemic preparedness through better, faster influenza vaccines. Expert Rev Vaccines 2021; 20:235–42. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
