

Lung cancer immunotherapy: progress, pitfalls, and promises
- PMID: 36810079
- PMCID: PMC9942077
- DOI: 10.1186/s12943-023-01740-y
Lung cancer immunotherapy: progress, pitfalls, and promises
Abstract
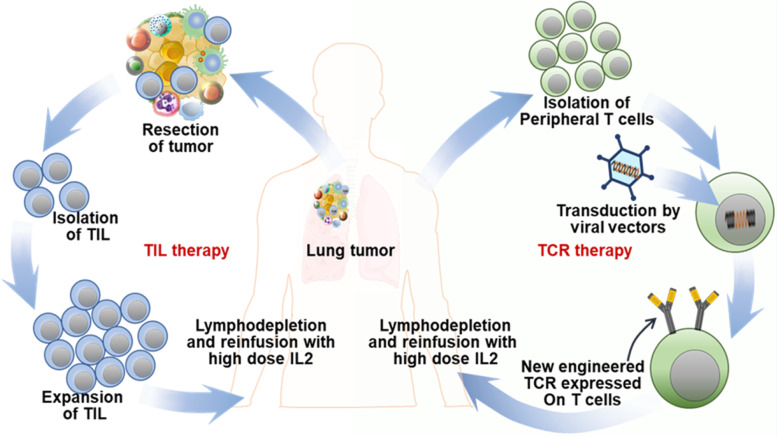
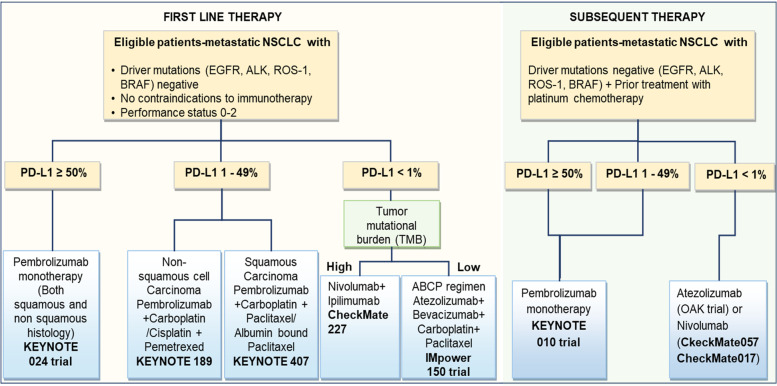
Lung cancer is the primary cause of mortality in the United States and around the globe. Therapeutic options for lung cancer treatment include surgery, radiation therapy, chemotherapy, and targeted drug therapy. Medical management is often associated with the development of treatment resistance leading to relapse. Immunotherapy is profoundly altering the approach to cancer treatment owing to its tolerable safety profile, sustained therapeutic response due to immunological memory generation, and effectiveness across a broad patient population. Different tumor-specific vaccination strategies are gaining ground in the treatment of lung cancer. Recent advances in adoptive cell therapy (CAR T, TCR, TIL), the associated clinical trials on lung cancer, and associated hurdles are discussed in this review. Recent trials on lung cancer patients (without a targetable oncogenic driver alteration) reveal significant and sustained responses when treated with programmed death-1/programmed death-ligand 1 (PD-1/PD-L1) checkpoint blockade immunotherapies. Accumulating evidence indicates that a loss of effective anti-tumor immunity is associated with lung tumor evolution. Therapeutic cancer vaccines combined with immune checkpoint inhibitors (ICI) can achieve better therapeutic effects. To this end, the present article encompasses a detailed overview of the recent developments in the immunotherapeutic landscape in targeting small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). Additionally, the review also explores the implication of nanomedicine in lung cancer immunotherapy as well as the combinatorial application of traditional therapy along with immunotherapy regimens. Finally, ongoing clinical trials, significant obstacles, and the future outlook of this treatment strategy are also highlighted to boost further research in the field.
Keywords: Adaptive cell therapy; Antibody; CAR T therapy; Cancer Vaccine; Immunomodulators; Immunotherapy; Lung Cancer; NSCLC; Nanomedicine; SCLC; TCR T therapy; TIL therapy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- American Cancer Society. Cancer Facts and Figures 2015. 2015. https://www.cancer.org/cancer-facts-and-figures-2015.pdf.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
