

Distinct Subtypes of Hepatorenal Syndrome and Associated Outcomes as Identified by Machine Learning Consensus Clustering
- PMID: 36810532
- PMCID: PMC9944494
- DOI: 10.3390/diseases11010018
Distinct Subtypes of Hepatorenal Syndrome and Associated Outcomes as Identified by Machine Learning Consensus Clustering
Abstract
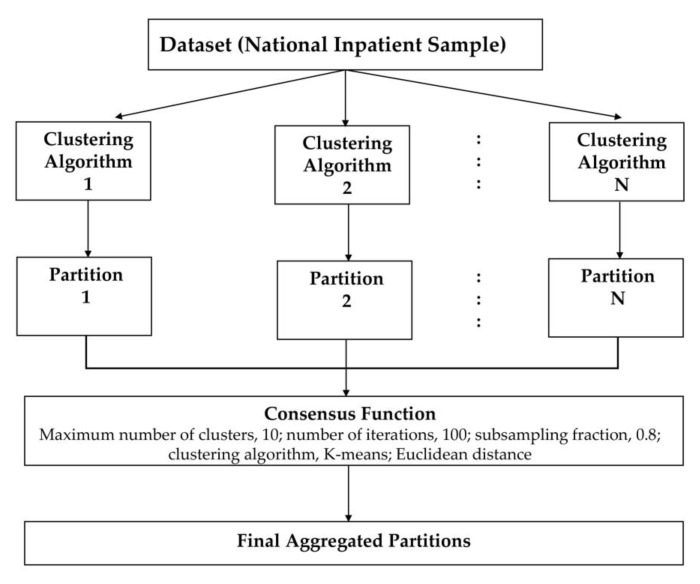
Background: The utilization of multi-dimensional patient data to subtype hepatorenal syndrome (HRS) can individualize patient care. Machine learning (ML) consensus clustering may identify HRS subgroups with unique clinical profiles. In this study, we aim to identify clinically meaningful clusters of hospitalized patients for HRS using an unsupervised ML clustering approach.
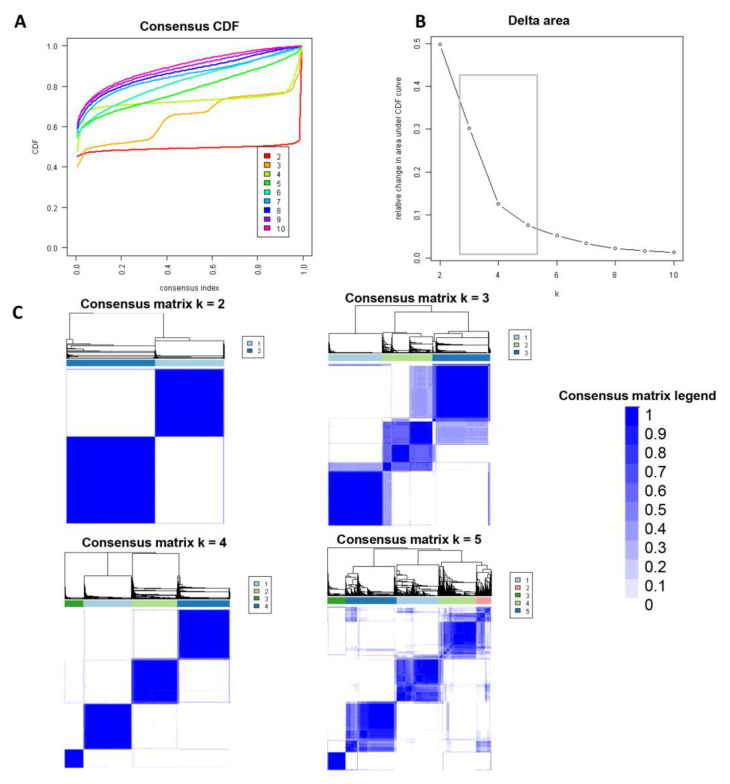
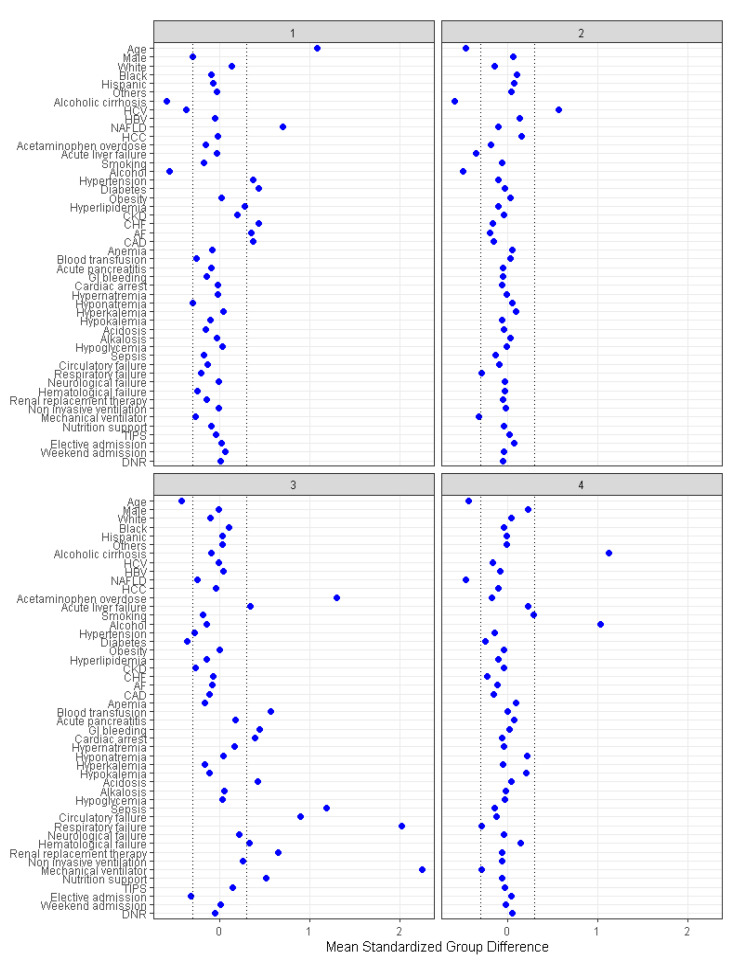
Methods: Consensus clustering analysis was performed based on patient characteristics in 5564 patients primarily admitted for HRS in the National Inpatient Sample from 2003-2014 to identify clinically distinct HRS subgroups. We applied standardized mean difference to evaluate key subgroup features, and compared in-hospital mortality between assigned clusters.
Results: The algorithm revealed four best distinct HRS subgroups based on patient characteristics. Cluster 1 patients (n = 1617) were older, and more likely to have non-alcoholic fatty liver disease, cardiovascular comorbidities, hypertension, and diabetes. Cluster 2 patients (n = 1577) were younger and more likely to have hepatitis C, and less likely to have acute liver failure. Cluster 3 patients (n = 642) were younger, and more likely to have non-elective admission, acetaminophen overdose, acute liver failure, to develop in-hospital medical complications and organ system failure, and to require supporting therapies, including renal replacement therapy, and mechanical ventilation. Cluster 4 patients (n = 1728) were younger, and more likely to have alcoholic cirrhosis and to smoke. Thirty-three percent of patients died in hospital. In-hospital mortality was higher in cluster 1 (OR 1.53; 95% CI 1.31-1.79) and cluster 3 (OR 7.03; 95% CI 5.73-8.62), compared to cluster 2, while cluster 4 had comparable in-hospital mortality (OR 1.13; 95% CI 0.97-1.32).
Conclusions: Consensus clustering analysis provides the pattern of clinical characteristics and clinically distinct HRS phenotypes with different outcomes.
Keywords: AKI; HRS; acute kidney injury; cirrhosis; clustering; hepatorenal syndrome; machine learning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Clinically Distinct Subtypes of Acute Kidney Injury on Hospital Admission Identified by Machine Learning Consensus Clustering.Med Sci (Basel). 2021 Sep 24;9(4):60. doi: 10.3390/medsci9040060. Med Sci (Basel). 2021. PMID: 34698185 Free PMC article.
-
Machine Learning Consensus Clustering Approach for Patients with Lactic Acidosis in Intensive Care Units.J Pers Med. 2021 Nov 2;11(11):1132. doi: 10.3390/jpm11111132. J Pers Med. 2021. PMID: 34834484 Free PMC article.
-
Machine Learning Consensus Clustering Approach for Hospitalized Patients with Phosphate Derangements.J Clin Med. 2021 Sep 27;10(19):4441. doi: 10.3390/jcm10194441. J Clin Med. 2021. PMID: 34640457 Free PMC article.
-
Acute kidney injury in acute-on-chronic liver failure: where does hepatorenal syndrome fit?Kidney Int. 2017 Nov;92(5):1058-1070. doi: 10.1016/j.kint.2017.04.048. Epub 2017 Aug 23. Kidney Int. 2017. PMID: 28844314 Review.
-
Epidemiology, Pathophysiology, and Management of Hepatorenal Syndrome.Semin Nephrol. 2019 Jan;39(1):17-30. doi: 10.1016/j.semnephrol.2018.10.002. Semin Nephrol. 2019. PMID: 30606404 Review.
References
-
- Fagundes C., Barreto R., Guevara M., Garcia E., Solà E., Rodríguez E., Graupera I., Ariza X., Pereira G., Alfaro I., et al. A modified acute kidney injury classification for diagnosis and risk stratification of impairment of kidney function in cirrhosis. J. Hepatol. 2013;59:474–481. doi: 10.1016/j.jhep.2013.04.036. - DOI - PubMed
LinkOut - more resources
Full Text Sources
