

Middle lobe suffering due to malposition and 180° tilt of the 2 remaining lobes after right upper lobectomy
- PMID: 36810693
- PMCID: PMC9976767
- DOI: 10.1093/icvts/ivad038
Middle lobe suffering due to malposition and 180° tilt of the 2 remaining lobes after right upper lobectomy
Abstract
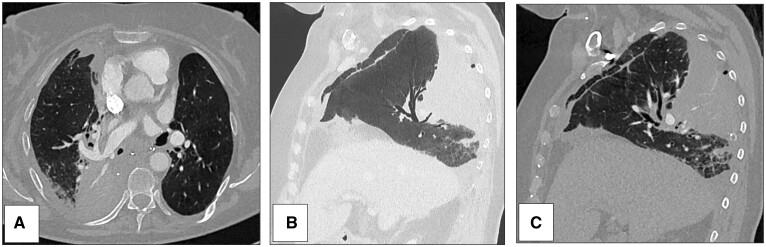
Middle lobe (ML) suffering after right upper lobectomy (RUL) is rare but represents a major complication usually due to lobar torsion. We report 3 atypical consecutive cases of ML suffering due to malposition of the 2 remaining right lobes with a 180° tilt. All 3 female patients had surgery for non-small-cell carcinoma including RUL associated with radical hilar and mediastinal lymph node removal. Postoperative chest X-ray abnormalities appeared at days 1-3 respectively. The diagnosis of malposition of the 2 lobes was done on contrast-enhanced chest CT scan at days 7, 7 and 6, respectively. A reoperation for suspected ML torsion was required in all patients. Three repositionings of the 2 lobes and 1 middle lobectomy were performed. The postoperative courses were then uneventful, and the 3 patients were alive at a mean follow-up of 12 months. Before thoracic approach closure after RUL, systematic check of good positioning of the 2 reinflated remaining lobes is indispensable. It may prevent ML suffering secondary to 180° lobar tilt leading to whole pulmonary malposition.
Keywords: Lobar malposition; Lung cancer; Middle lobe suffering; Morbidity; Postoperative; Right upper lobectomy.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures

References
-
- Epplen F, Jacobson AL.. Twisted pedicle of accessory lobe of the lung. JAMA 1930;94:1135.
-
- Dai J, Xie D, Wang H, He W, Zhou Y, Hernández-Arenas LA. et al. Predictors of survival in lung torsion: a systematic review and pooled analysis. J Thorac Cardiovasc Surg 2016;152:737–45.e3. - PubMed
-
- Moser ES, Proto AV.. Lung torsion: case report and literature review. Radiology 1987;162:639–43. - PubMed
-
- Hennink S, Wouters MWJM, Klomp HM, Baas P.. Necrotizing pneumonitis caused by postoperative pulmonary torsion. Interdisc CardioVasc Thorac Surg 2008;7:144–5. - PubMed
LinkOut - more resources
Full Text Sources
