

Symptom severity trajectories and distresses in patients undergoing video-assisted thoracoscopic lung resection from surgery to the first post-discharge clinic visit
- PMID: 36812255
- PMCID: PMC9946218
- DOI: 10.1371/journal.pone.0281998
Symptom severity trajectories and distresses in patients undergoing video-assisted thoracoscopic lung resection from surgery to the first post-discharge clinic visit
Abstract
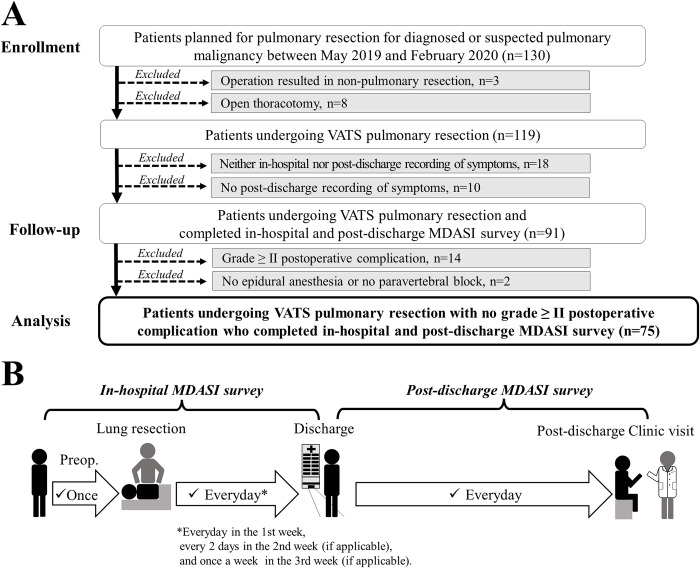
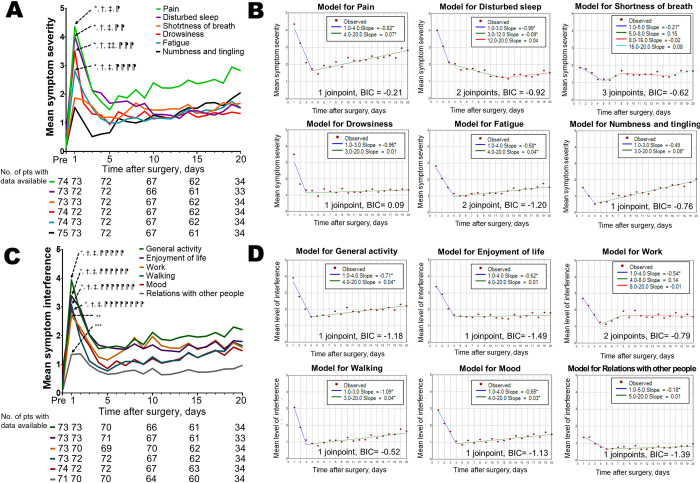
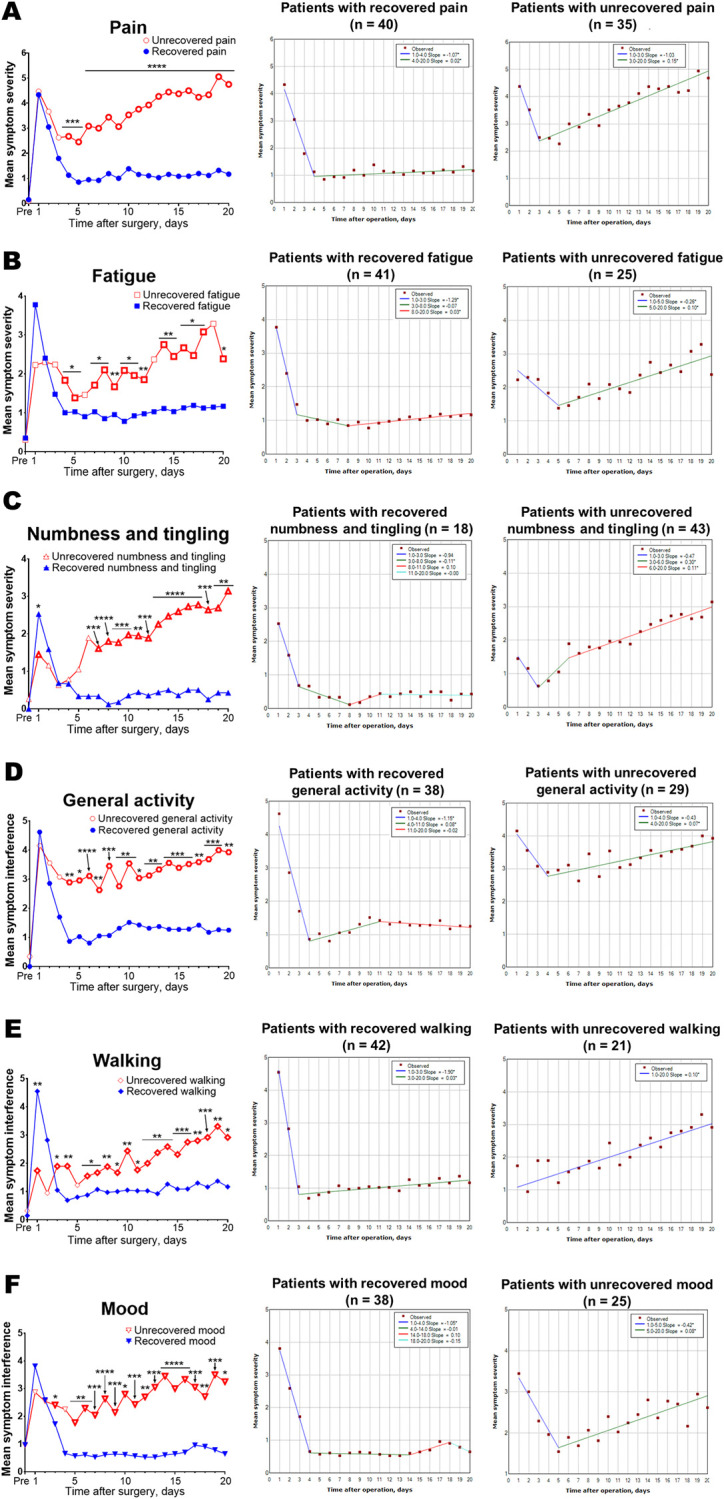
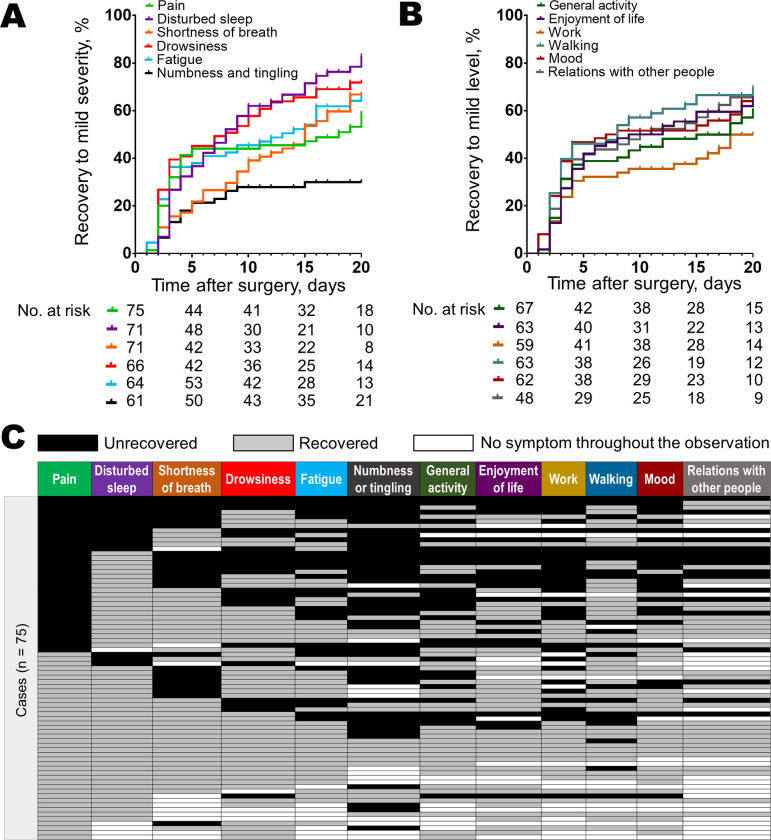
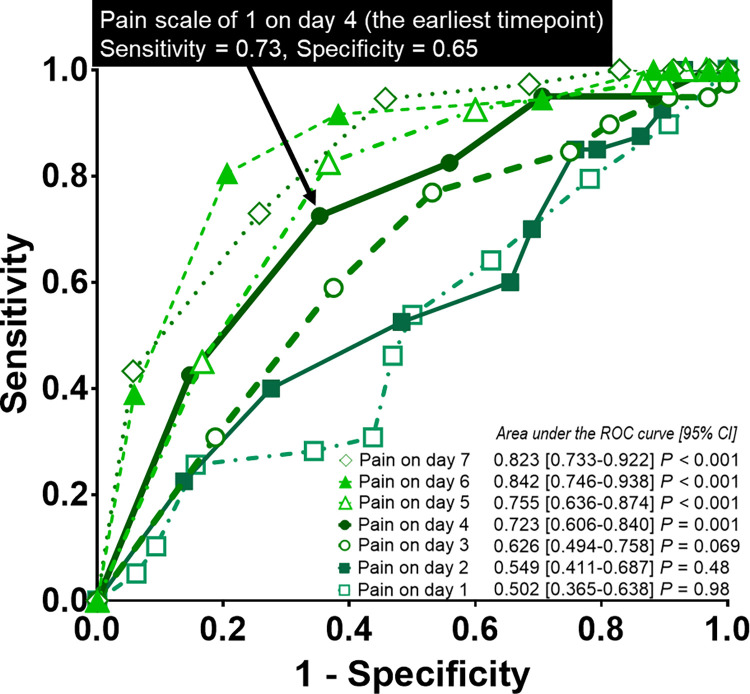
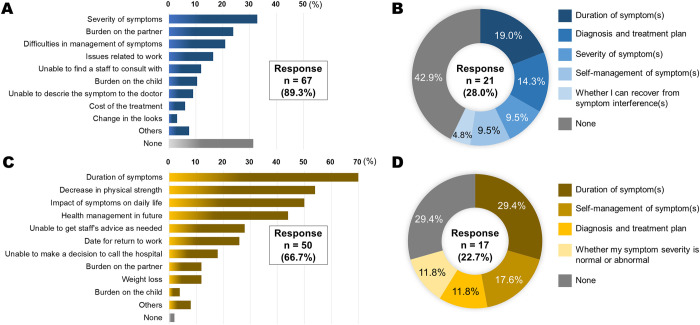
This study aimed to characterize patients' symptom severity trajectories and distresses from video-assisted thoracoscopic lung resection to the first post-discharge clinic visit. Seventy-five patients undergoing thoracoscopic lung resection for diagnosed or suspected pulmonary malignancy prospectively recorded daily symptom severity on a 0-10 numeric scale using the MD Anderson Symptom Inventory until the first post-discharge clinic visit. The causes of postoperative distresses were surveyed, and symptom severity trajectories were analyzed using joinpoint regression. A rebound was defined as a statistically significant positive slope after a statistically significant negative slope. Symptom recovery was defined as symptom severity of ≤3 in two contiguous measurements. The accuracy of pain severity on days 1-5 for predicting pain recovery was determined using area under the receiver operating characteristic curves. We applied Cox proportional hazards models for multivariate analyses of the potential predictors of early pain recovery. The median age was 70 years, and females accounted for 48%. The median interval from surgery to the first post-discharge clinic visit was 20 days. Trajectories of several core symptoms including pain showed a rebound from day 3 or 4. Specifically, pain severity in patients with unrecovered pain had been higher than those with recovered pain since day 4. Pain severity on day 4 showed the highest area under the curve of 0.723 for predicting pain recovery (P = 0.001). Multivariate analysis identified pain severity of ≤1 on day 4 as an independent predictor of early pain recovery (hazard ratio, 2.86; P = 0.0027). Duration of symptom was the leading cause of postoperative distress. Several core symptoms after thoracoscopic lung resection showed a rebound in the trajectory. Specifically, a rebound in pain trajectory may be associated with unrecovered pain; pain severity on day 4 may predict early pain recovery. Further clarification of symptom severity trajectories is essential for patient-centered care.
Copyright: © 2023 Saito et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Symptom recovery after thoracic surgery: Measuring patient-reported outcomes with the MD Anderson Symptom Inventory.J Thorac Cardiovasc Surg. 2015 Sep;150(3):613-9.e2. doi: 10.1016/j.jtcvs.2015.05.057. Epub 2015 May 28. J Thorac Cardiovasc Surg. 2015. PMID: 26088408 Free PMC article.
-
Establishment of Minimal Clinically Important Improvement for Patient-Reported Symptoms to Define Recovery After Video-Assisted Thoracoscopic Surgery.Ann Surg Oncol. 2022 Sep;29(9):5593-5604. doi: 10.1245/s10434-022-11629-7. Epub 2022 Apr 3. Ann Surg Oncol. 2022. PMID: 35368219
-
Functional recovery after discharge in enhanced recovery video-assisted thoracoscopic lobectomy: a pilot prospective cohort study.Anaesthesia. 2022 May;77(5):555-561. doi: 10.1111/anae.15682. Epub 2022 Mar 8. Anaesthesia. 2022. PMID: 35261025
-
Ventilatory efficiency slope is associated with cardiopulmonary complications after thoracoscopic anatomical lung resection.Interact Cardiovasc Thorac Surg. 2022 Jun 15;35(1):ivac039. doi: 10.1093/icvts/ivac039. Interact Cardiovasc Thorac Surg. 2022. PMID: 35157073 Free PMC article. Review.
-
Impact of video-assisted thoracoscopic major lung resection on immune function.Asian Cardiovasc Thorac Ann. 2009 Aug;17(4):426-32. doi: 10.1177/0218492309338100. Asian Cardiovasc Thorac Ann. 2009. PMID: 19713346 Review.
Cited by
-
Diagnostic Dilemma of Rounded Atelectasis in the Left Lower Lobe Showing High Uptake of 18F-Fluorodeoxyglucose: A Surgical Conundrum.Cureus. 2025 Apr 25;17(4):e83005. doi: 10.7759/cureus.83005. eCollection 2025 Apr. Cureus. 2025. PMID: 40416114 Free PMC article.
-
SCAPAS-LungCancer-improving supportive care for patients surgically treated for non-small cell lung cancer: protocol for a prospective, longitudinal, observational and exploratory multicentre study.BMJ Open. 2025 Apr 23;15(4):e094823. doi: 10.1136/bmjopen-2024-094823. BMJ Open. 2025. PMID: 40268490 Free PMC article.
References
-
- Committee for Scientific Affairs, The Japanese Association for Thoracic Surgery, Shimizu H, Endo S, Natsugoe S, Doki Y, et al.. Thoracic and cardiovascular surgery in Japan in 2016: annual report by the Japanese Association for Thoracic Surgery. Gen Thorac Cardiovasc Surg. 2019;67: 377–411. doi: 10.1007/s11748-019-01068-9 - DOI - PubMed
-
- Yamaguchi K, Joint Study Group on the Sociology of Cancer. A report on research into the anxieties and burdens of cancer sufferers − the views of 7885 people who faced up to cancer; 2004. Nagaizumi-Chou [Cited 2022 January 10]. Available from: http://www.scchr.jp/yorozu/pdf/taiken_koe_eng.pdf (English version). Shizuoka: Shizuoka Cancer Center.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
