

The Cooperative Re-Engagement Controlled Trial (CoRECT): Durable Viral Suppression Assessment
- PMID: 36812382
- PMCID: PMC10962216
- DOI: 10.1097/QAI.0000000000003178
The Cooperative Re-Engagement Controlled Trial (CoRECT): Durable Viral Suppression Assessment
Abstract
Background: A collaborative, data-to-care strategy to identify persons with HIV (PWH) newly out-of-care, combined with an active public health intervention, significantly increases the proportion of PWH re-engaged in HIV care. We assessed this strategy's impact on durable viral suppression (DVS).
Methods: A multisite, prospective randomized controlled trial for out-of-care individuals using a data-to-care strategy and comparing public health field services to locate, contact, and facilitate access to care versus the standard of care. DVS was defined as the last viral load, the viral load at least 3 months before, and any viral load between the 2 were all <200 copies/mL during the 18-month postrandomization. Alternative definitions of DVS were also analyzed.
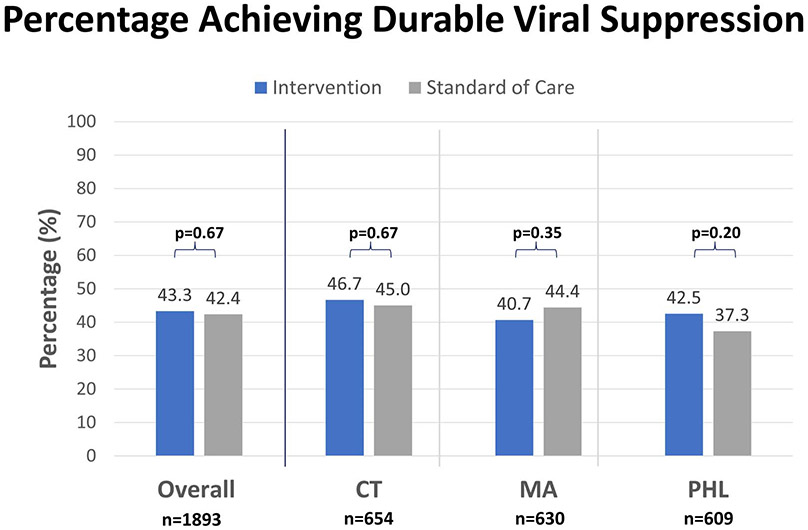
Results: Between August 1, 2016-July 31, 2018, 1893 participants were randomized from Connecticut (n = 654), Massachusetts (n = 630), and Philadelphia (n = 609). Rates of achieving DVS were similar in the intervention and standard-of-care arms in all jurisdictions (all sites: 43.4% vs 42.4%, P = 0.67; Connecticut: 46.7% vs 45.0%, P = 0.67; Massachusetts: 40.7 vs 44.4%, P = 0.35; Philadelphia: 42.4% vs 37.3%, P = 0.20). There was no association between DVS and the intervention (RR: 1.01, CI: 0.91-1.12; P = 0.85) adjusting for site, age categories, race/ethnicity, birth sex, CD4 categories, and exposure categories.
Conclusion: A collaborative, data-to-care strategy, and active public health intervention did not increase the proportion of PWH achieving DVS, suggesting additional support to promote retention in care and antiretroviral adherence may be needed. Initial linkage and engagement services, through data-to-care or other means, are likely necessary but insufficient for achieving DVS for all PWH.
Trial registration: ClinicalTrials.gov NCT02693145.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Figures
References
-
- Centers for Disease Control and Prevention. Monitoring Selected National HIV Prevention and Care Objectives by Using HIV Surveillance Data—United States and 6 Dependent Areas, 2019. HIV Surveillance Supplemental Report; 2021;26(No.2). Available at: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html.No.2
-
- The White House. National HIV/AIDS Strategy for the United States 2022–2025. Washington, DC; 2021. Available at: https://www.whitehouse.gov/wp-content/uploads/2021/11/National-HIV-AIDS-...
-
- Skarbinski J, Rosenberg E, Paz-Bailey G, et al. Human immunodeficiency virus transmission at each step of the care continuum in the United States. JAMA Intern Med. 2015;175:588–596. - PubMed
-
- Murphy EL, Collier AC, Kalish LA, et al. Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med. 2001; 135:17–26. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
