

Unifying cardiovascular modelling with deep reinforcement learning for uncertainty aware control of sepsis treatment
- PMID: 36812511
- PMCID: PMC9931225
- DOI: 10.1371/journal.pdig.0000012
Unifying cardiovascular modelling with deep reinforcement learning for uncertainty aware control of sepsis treatment
Abstract
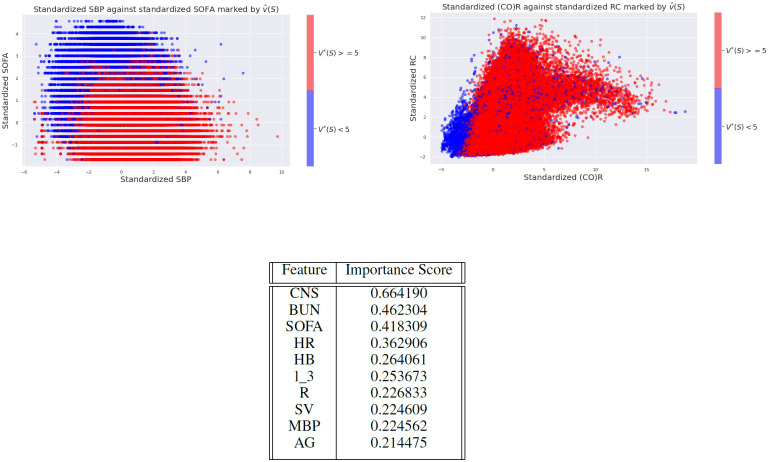
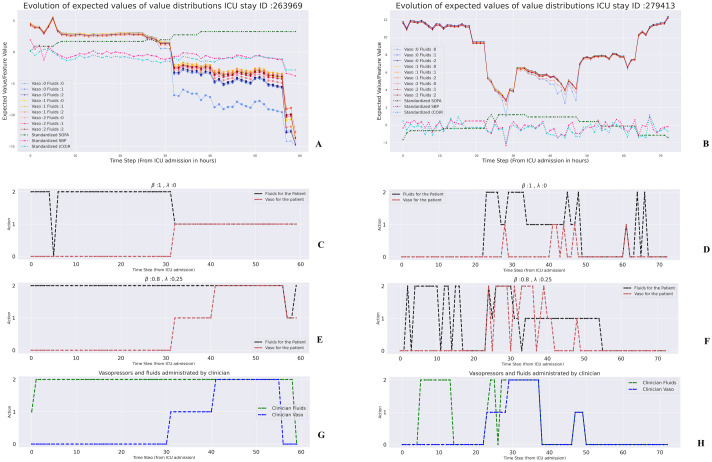
Sepsis is a potentially life-threatening inflammatory response to infection or severe tissue damage. It has a highly variable clinical course, requiring constant monitoring of the patient's state to guide the management of intravenous fluids and vasopressors, among other interventions. Despite decades of research, there's still debate among experts on optimal treatment. Here, we combine for the first time, distributional deep reinforcement learning with mechanistic physiological models to find personalized sepsis treatment strategies. Our method handles partial observability by leveraging known cardiovascular physiology, introducing a novel physiology-driven recurrent autoencoder, and quantifies the uncertainty of its own results. Moreover, we introduce a framework for uncertainty-aware decision support with humans in the loop. We show that our method learns physiologically explainable, robust policies, that are consistent with clinical knowledge. Further our method consistently identifies high-risk states that lead to death, which could potentially benefit from more frequent vasopressor administration, providing valuable guidance for future research.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
LinkOut - more resources
Full Text Sources