

Is artificial intelligence capable of generating hospital discharge summaries from inpatient records?
- PMID: 36812600
- PMCID: PMC9931331
- DOI: 10.1371/journal.pdig.0000158
Is artificial intelligence capable of generating hospital discharge summaries from inpatient records?
Abstract
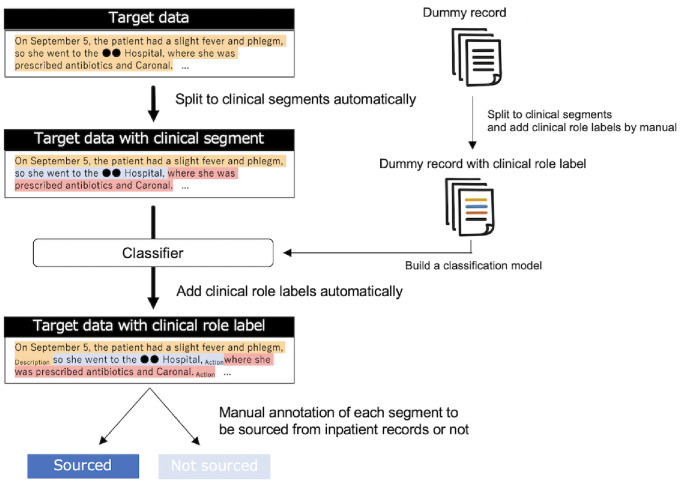
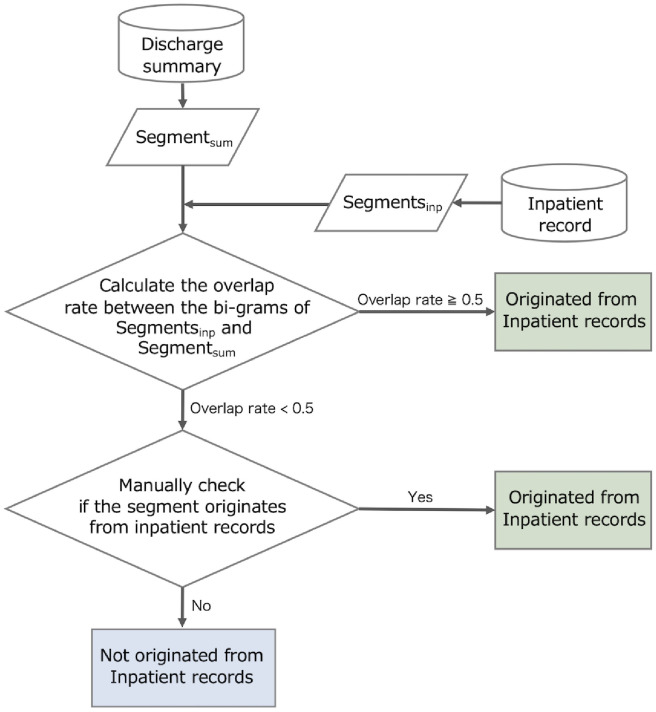
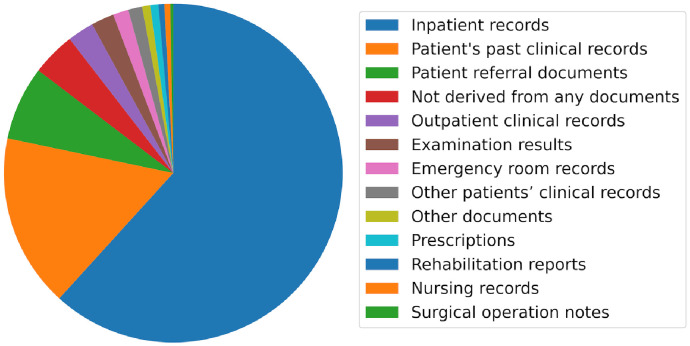
Medical professionals have been burdened by clerical work, and artificial intelligence may efficiently support physicians by generating clinical summaries. However, whether hospital discharge summaries can be generated automatically from inpatient records stored in electronic health records remains unclear. Therefore, this study investigated the sources of information in discharge summaries. First, the discharge summaries were automatically split into fine-grained segments, such as those representing medical expressions, using a machine learning model from a previous study. Second, these segments in the discharge summaries that did not originate from inpatient records were filtered out. This was performed by calculating the n-gram overlap between inpatient records and discharge summaries. The final source origin decision was made manually. Finally, to reveal the specific sources (e.g., referral documents, prescriptions, and physician's memory) from which the segments originated, they were manually classified by consulting medical professionals. For further and deeper analysis, this study designed and annotated clinical role labels that represent the subjectivity of the expressions and builds a machine learning model to assign them automatically. The analysis results revealed the following: First, 39% of the information in the discharge summary originated from external sources other than inpatient records. Second, patient's past clinical records constituted 43%, and patient referral documents constituted 18% of the expressions derived from external sources. Third, 11% of the missing information was not derived from any documents. These are possibly derived from physicians' memories or reasoning. According to these results, end-to-end summarization using machine learning is considered infeasible. Machine summarization with an assisted post-editing process is the best fit for this problem domain.
Copyright: © 2022 Ando et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare no conflicts of interest associated with this manuscript.
Figures

Similar articles
-
Exploring optimal granularity for extractive summarization of unstructured health records: Analysis of the largest multi-institutional archive of health records in Japan.PLOS Digit Health. 2022 Sep 15;1(9):e0000099. doi: 10.1371/journal.pdig.0000099. eCollection 2022 Sep. PLOS Digit Health. 2022. PMID: 36812582 Free PMC article.
-
Is the routine health information system ready to support the planned national health insurance scheme in South Africa?Health Policy Plan. 2021 Jun 1;36(5):639-650. doi: 10.1093/heapol/czab008. Health Policy Plan. 2021. PMID: 33822055 Free PMC article.
-
Nurses engaging with referral letters and discharge summaries: A qualitative study.J Clin Nurs. 2024 Jun;33(6):2309-2323. doi: 10.1111/jocn.17054. Epub 2024 Feb 2. J Clin Nurs. 2024. PMID: 38304996
-
Facilitating the Information Exchange Using a Modular Electronic Discharge Summary.Stud Health Technol Inform. 2018;248:72-79. Stud Health Technol Inform. 2018. PMID: 29726421 Review.
-
Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care.JAMA. 2007 Feb 28;297(8):831-41. doi: 10.1001/jama.297.8.831. JAMA. 2007. PMID: 17327525 Review.
Cited by
-
Using ChatGPT for writing hospital inpatient discharge summaries - perspectives from an inpatient infectious diseases service.BMC Health Serv Res. 2025 Feb 10;25(1):221. doi: 10.1186/s12913-025-12373-w. BMC Health Serv Res. 2025. PMID: 39924512 Free PMC article.
-
Automated generation of discharge summaries: leveraging large language models with clinical data.Sci Rep. 2025 May 12;15(1):16466. doi: 10.1038/s41598-025-01618-7. Sci Rep. 2025. PMID: 40355506 Free PMC article.
-
ChatGPT in Plastic and Reconstructive Surgery.Indian J Plast Surg. 2023 Aug 2;56(4):320-325. doi: 10.1055/s-0043-1771514. eCollection 2023 Aug. Indian J Plast Surg. 2023. PMID: 37705820 Free PMC article. Review.
-
Improving specialist palliative care discharges from hospitals and hospices to community settings: a qualitative interview study of the communication experiences of patients, carers, and primary care professionals.BMC Palliat Care. 2025 Jul 26;24(1):214. doi: 10.1186/s12904-025-01851-x. BMC Palliat Care. 2025. PMID: 40713648 Free PMC article.
-
Optimizing Discharge Summaries: A Survey of Inpatient Clinician Perspectives and the Path to Standardization.J Gen Intern Med. 2025 Jul 25. doi: 10.1007/s11606-025-09740-y. Online ahead of print. J Gen Intern Med. 2025. PMID: 40711633
References
LinkOut - more resources
Full Text Sources
Miscellaneous