

Informing antimicrobial stewardship with explainable AI
- PMID: 36812617
- PMCID: PMC9931350
- DOI: 10.1371/journal.pdig.0000162
Informing antimicrobial stewardship with explainable AI
Abstract
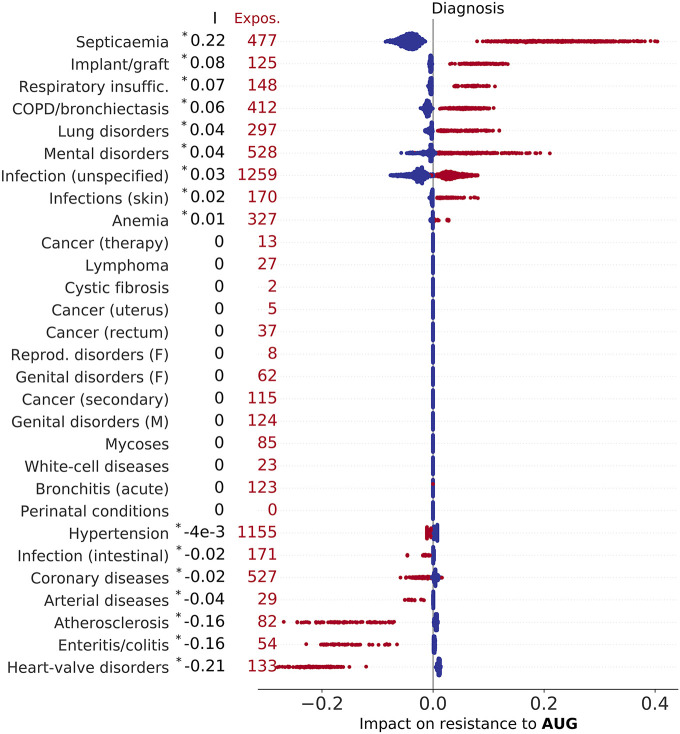
The accuracy and flexibility of artificial intelligence (AI) systems often comes at the cost of a decreased ability to offer an intuitive explanation of their predictions. This hinders trust and discourage adoption of AI in healthcare, exacerbated by concerns over liabilities and risks to patients' health in case of misdiagnosis. Providing an explanation for a model's prediction is possible due to recent advances in the field of interpretable machine learning. We considered a data set of hospital admissions linked to records of antibiotic prescriptions and susceptibilities of bacterial isolates. An appropriately trained gradient boosted decision tree algorithm, supplemented by a Shapley explanation model, predicts the likely antimicrobial drug resistance, with the odds of resistance informed by characteristics of the patient, admission data, and historical drug treatments and culture test results. Applying this AI-based system, we found that it substantially reduces the risk of mismatched treatment compared with the observed prescriptions. The Shapley values provide an intuitive association between observations/data and outcomes; the associations identified are broadly consistent with expectations based on prior knowledge from health specialists. The results, and the ability to attribute confidence and explanations, support the wider adoption of AI in healthcare.
Copyright: © 2023 Cavallaro et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Nicholson Price II W. Risks and remedies for artificial intelligence in health care. 2019. Available from: https://www.brookings.edu/research/risks-and-remedies-for-artificial-int... (Accessed 1/12/2022).
-
- Understanding healthcare workers’ confidence in AI. 2022. Available from: https://digital-transformation.hee.nhs.uk/building-a-digital-workforce/d... (Accessed 1/12/2022).
-
- Adadi A, Berrada M. Peeking Inside the Black-Box: A Survey on Explainable Artificial Intelligence (XAI). IEEE Access. 2018;6:52138–52160. doi: 10.1109/ACCESS.2018.2870052 - DOI
Grants and funding
LinkOut - more resources
Full Text Sources