

Diagnostic workup of childhood interstitial lung disease
- PMID: 36813289
- PMCID: PMC9945877
- DOI: 10.1183/16000617.0188-2022
Diagnostic workup of childhood interstitial lung disease
Abstract
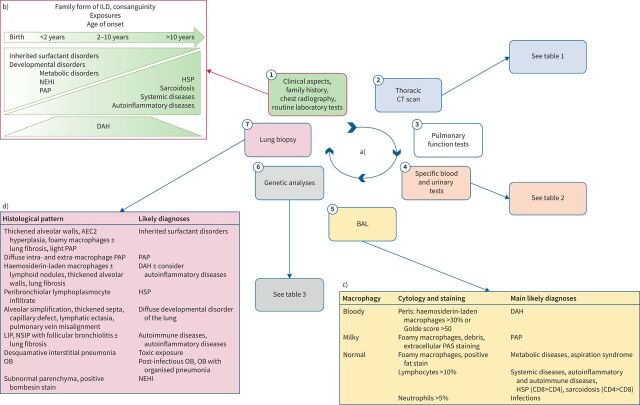
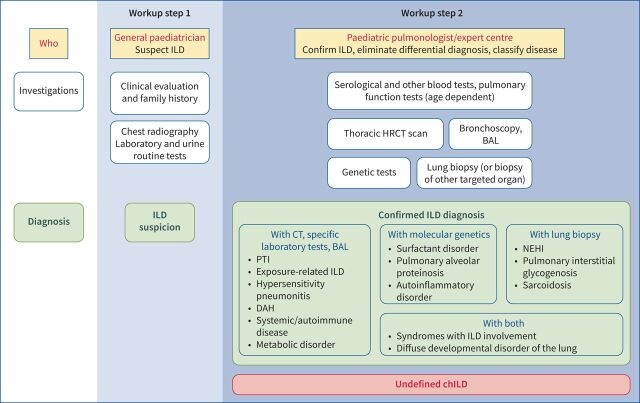
Childhood interstitial lung diseases (chILDs) are rare and heterogeneous diseases with significant morbidity and mortality. An accurate and quick aetiological diagnosis may contribute to better management and personalised treatment. On behalf of the European Respiratory Society Clinical Research Collaboration for chILD (ERS CRC chILD-EU), this review summarises the roles of the general paediatrician, paediatric pulmonologists and expert centres in the complex diagnostic workup. Each patient's aetiological chILD diagnosis must be reached without prolonged delays in a stepwise approach from medical history, signs, symptoms, clinical tests and imaging, to advanced genetic analysis and specialised procedures including bronchoalveolar lavage and biopsy, if necessary. Finally, as medical progress is fast, the need to revisit a diagnosis of "undefined chILD" is stressed.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Comment in
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical