

Analysis of clinical and genomic profiles of therapy-related myeloid neoplasm in Korea
- PMID: 36814285
- PMCID: PMC9948421
- DOI: 10.1186/s40246-023-00458-8
Analysis of clinical and genomic profiles of therapy-related myeloid neoplasm in Korea
Abstract
Background: Therapy-related myeloid neoplasm (T-MN) rarely occurs among cancer survivors, and was characterized by poor prognosis. T-MN has germline predisposition in a considerable proportion. Here, clinical characteristics and germline/somatic variant profiles in T-MN patients were investigated, and the findings were compared with those of previous studies.
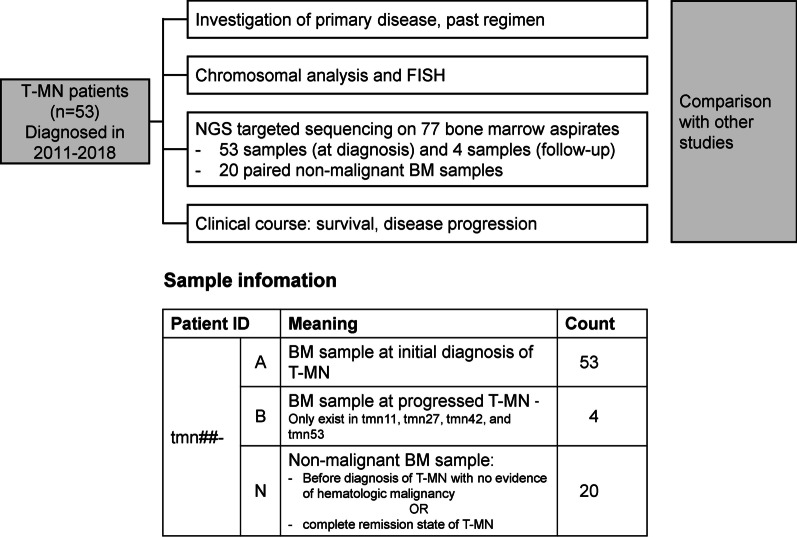
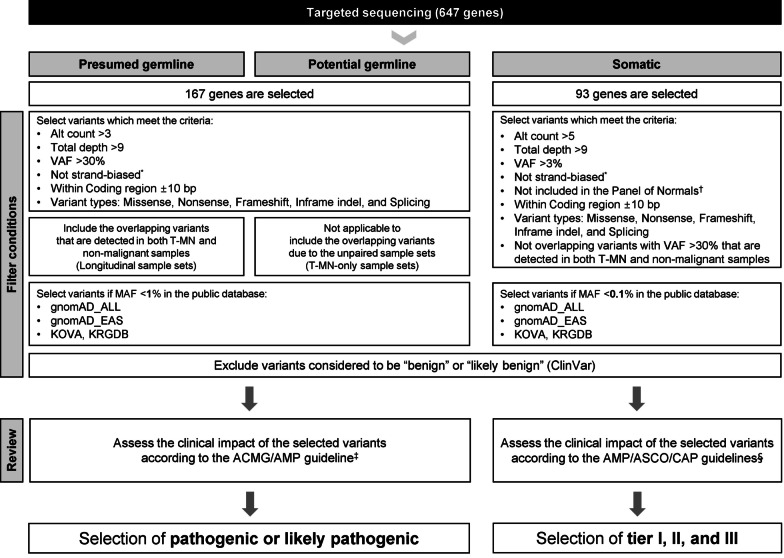
Methods: A review of medical records, cytogenetic study, targeted sequencing by next-generation sequencing, and survival analysis were performed on 53 patients with T-MN at a single institution in Korea.
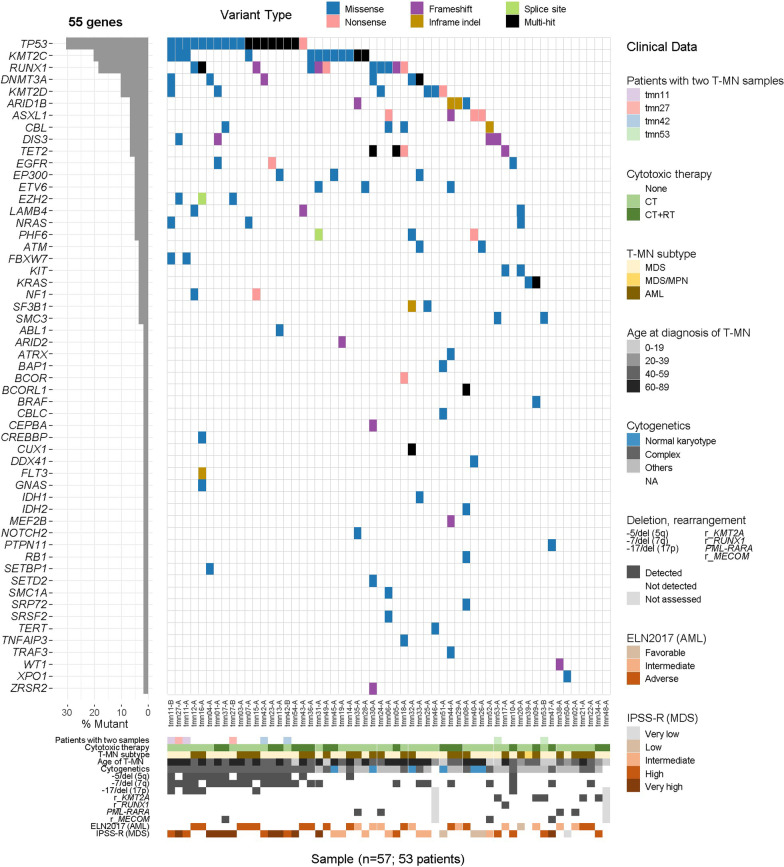
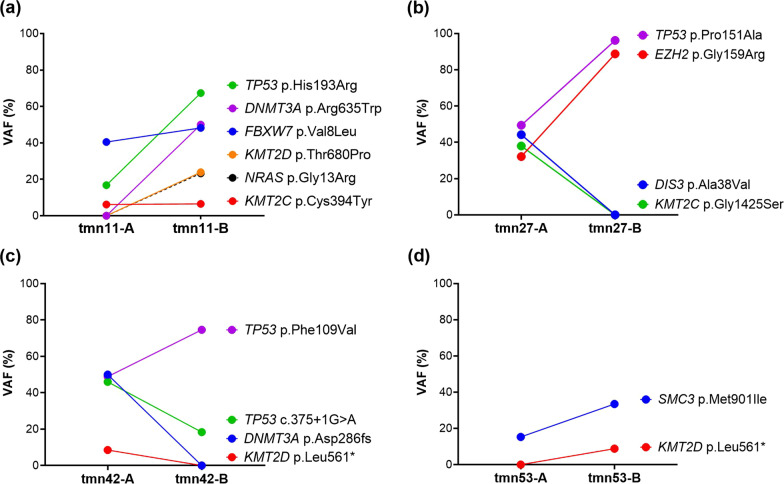
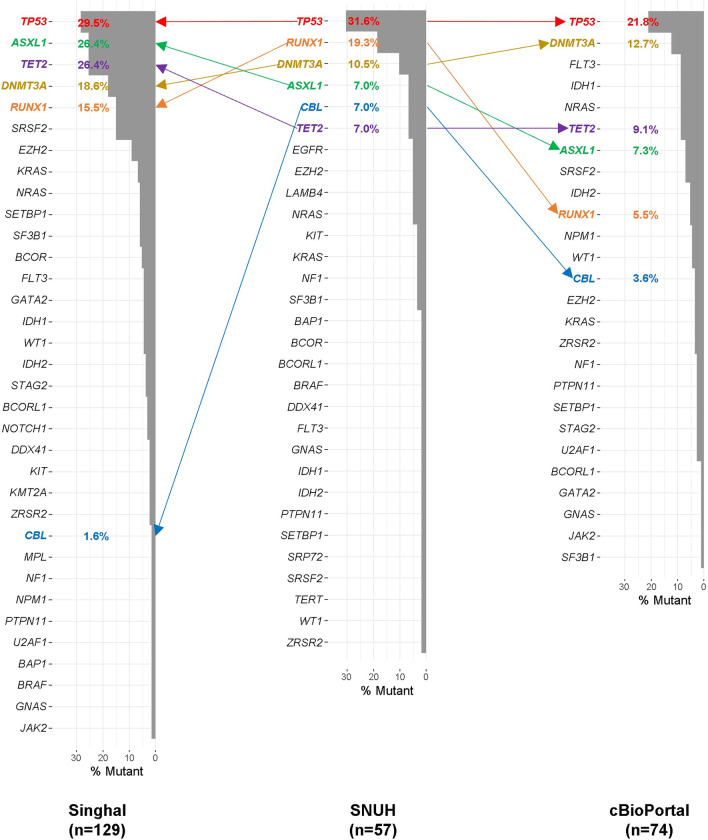
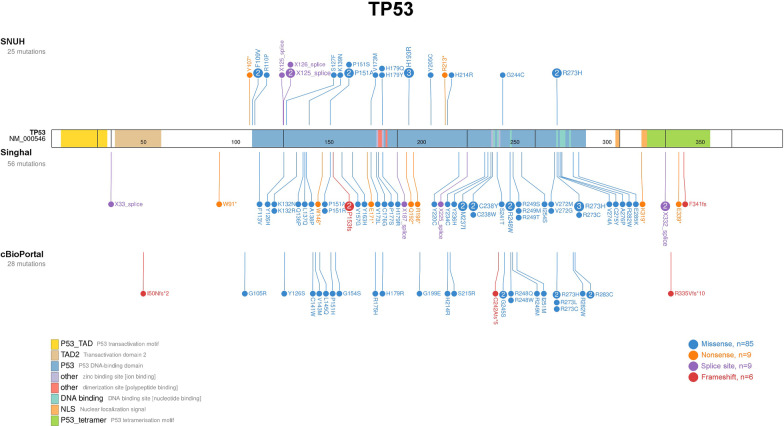
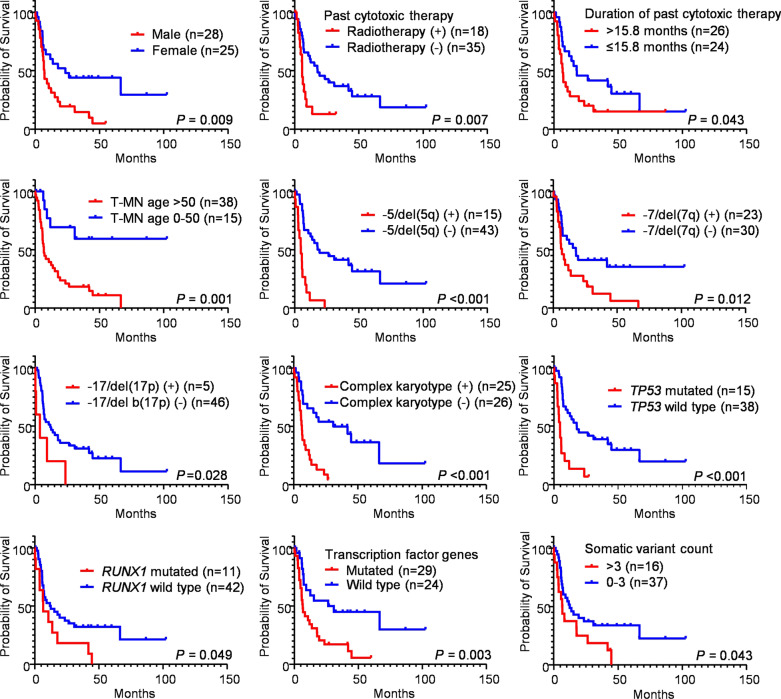
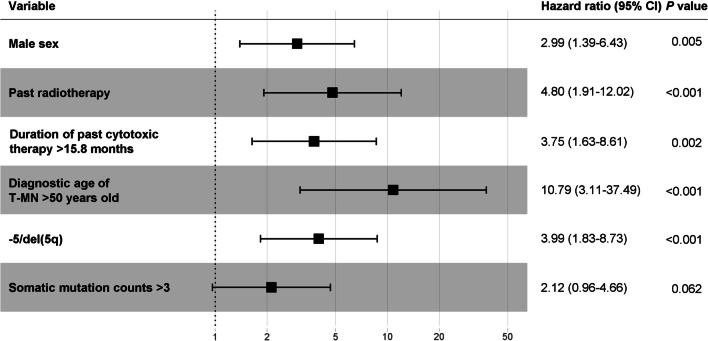
Results: The patients were relatively younger compared to T-MN patients in other studies. Our T-MN patients showed a high frequency of complex karyotypes, -5/del(5q), and -7/del(7q), which was similar to the Japanese study group but higher than the Australian study group. The most common primary disease was non-Hodgkin lymphoma, followed by breast cancer. The detailed distributions of primary diseases were different across study groups. Seven patients (13.2%) harbored deleterious presumed/potential germline variants in cancer predisposition genes (CPG) such as BRIP1, CEBPA, DDX41, FANCM, NBN, NF1, and RUNX1. In the somatic variant profile, TP53 was the most frequently mutated gene, which was consistent with the previous studies about T-MN. However, the somatic variant frequency in our study group was lower than in other studies. Adverse factors for overall survival were male sex, older age, history of previous radiotherapy, previous longer cytotoxic therapy, and -5/del(5q).
Conclusion: The findings of our study corroborate important information about T-MN patients. As well as a considerable predisposition to CPG, the clinical characteristics and somatic variant profile showed distinctive patterns. Germline variant testing should be recommended for T-MN patients. If the T-MN patients harbor pathogenic germline variants, the family members for stem cell donation should be screened for carrier status through germline variant testing to avoid donor-derived myeloid neoplasm. For the prediction of the prognosis in T-MN patients, sex, age, past treatment history, and cytogenetic findings can be considered.
Keywords: Germline predisposition; Next-generation sequencing; Somatic mutation; Therapy-related myeloid neoplasm.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no potential competing interests.
Figures
References
-
- Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al., editors. WHO classification of tumours of haematopoietic and lymphoid tissues. 4. Lyon: International Agency for Research on Cancer; 2017.
-
- Hulegårdh E, Nilsson C, Lazarevic V, Garelius H, Antunovic P, Rangert Derolf Å, et al. Characterization and prognostic features of secondary acute myeloid leukemia in a population-based setting: a report from the Swedish Acute Leukemia Registry. Am J Hematol. 2015;90(3):208–214. doi: 10.1002/ajh.23908. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
