

Novel regenerative drug, SPG302 promotes functional recovery of diaphragm muscle activity after cervical spinal cord injury
- PMID: 36815402
- PMCID: PMC10404468
- DOI: 10.1113/JP284004
Novel regenerative drug, SPG302 promotes functional recovery of diaphragm muscle activity after cervical spinal cord injury
Abstract
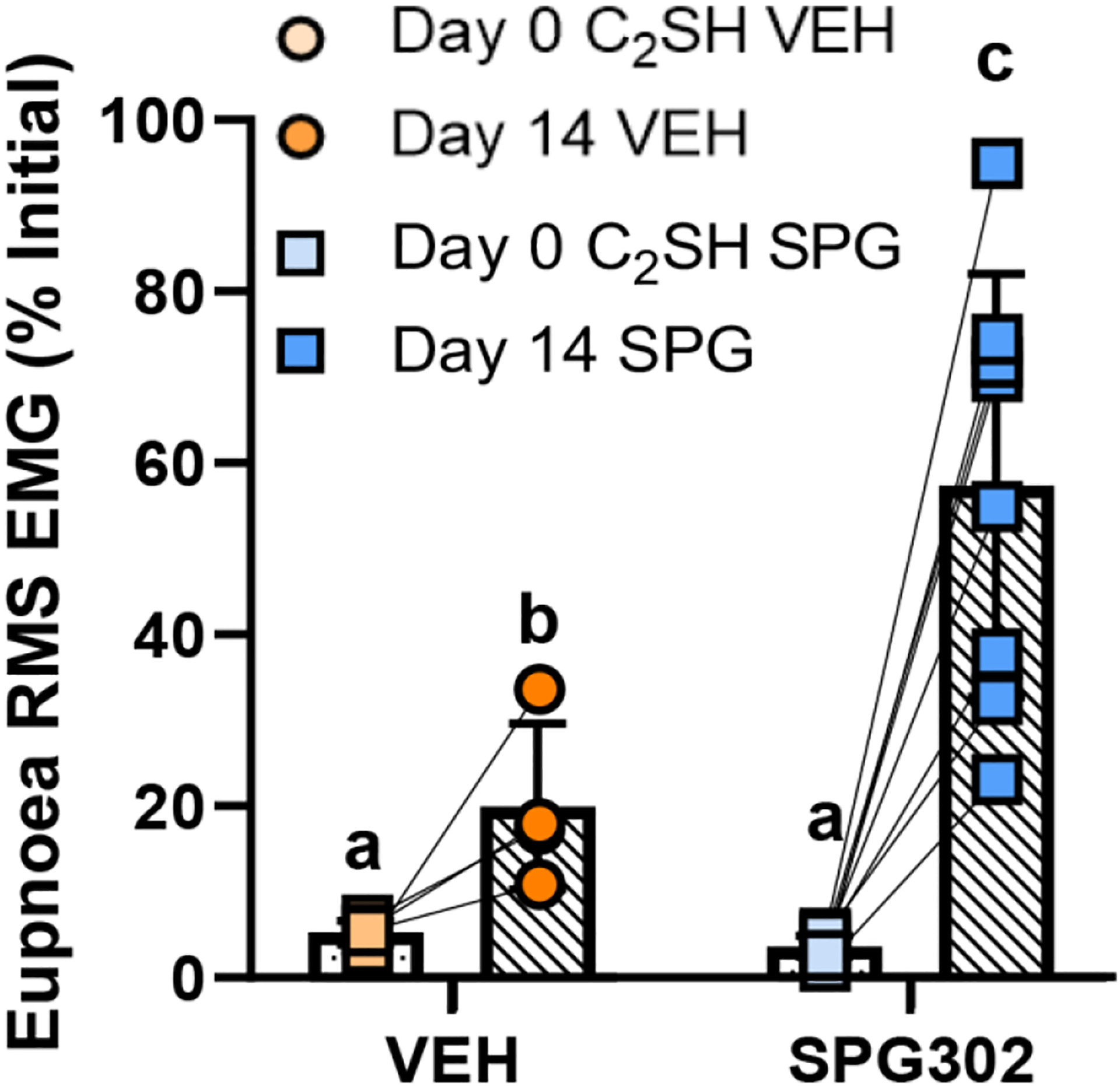
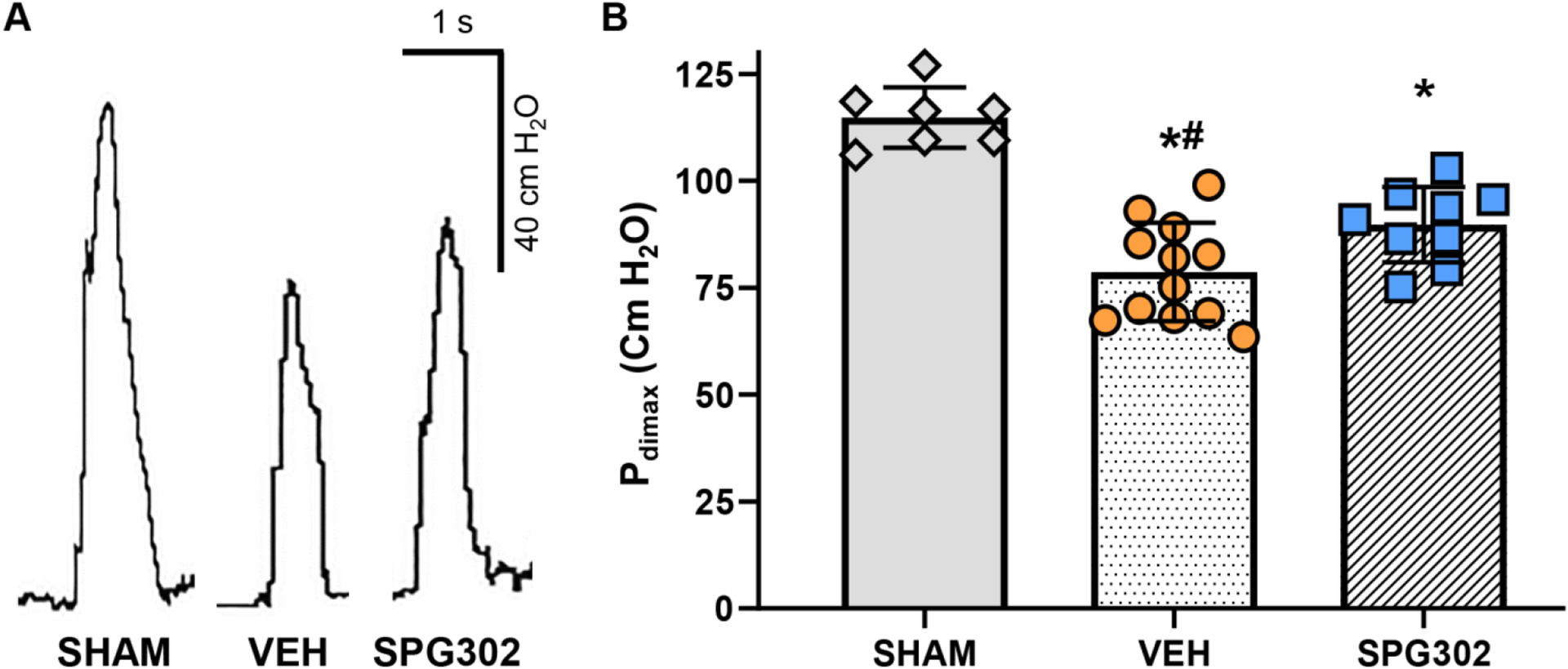
Spinal cord hemisection at C2 (C2 SH), sparing the dorsal column is widely used to investigate the effects of reduced phrenic motor neuron (PhMN) activation on diaphragm muscle (DIAm) function, with reduced DIAm activity on the injured side during eupnoea. Following C2 SH, recovery of DIAm EMG activity may occur spontaneously over subsequent days/weeks. Various strategies have been effective at improving the incidence and magnitude of DIAm recovery during eupnoea, but little is known about the effects of C2 SH on transdiaphragmatic pressure (Pdi ) during other ventilatory and non-ventilatory behaviours. We employ SPG302, a novel type of pegylated benzothiazole derivative, to assess whether enhancing synaptogenesis (i.e., enhancing spared local connections) will improve the incidence and the magnitude of recovery of DIAm EMG activity and Pdi function 14 days post-C2 SH. In anaesthetised Sprague-Dawley rats, DIAm EMG and Pdi were assessed during eupnoea, hypoxia/hypercapnia and airway occlusion prior to surgery (C2 SH or sham), immediately post-surgery and at 14 days post-surgery. In C2 SH rats, 14 days of DMSO (vehicle) or SPG302 treatments (i.p. injection) occurred. At the terminal experiment, maximum Pdi was evoked by bilateral phrenic nerve stimulation. We show that significant EMG and Pdi deficits are apparent in C2 SH compared with sham rats immediately after surgery. In C2 SH rats treated with SPG302, recovery of eupneic, hypoxia/hypercapnia and occlusion DIAm EMG was enhanced compared with vehicle rats after 14 days. Treatment with SPG302 also ameliorated Pdi deficits following C2 SH. In summary, SPG302 is an exciting new therapy to explore for use in spinal cord injuries. KEY POINTS: Despite advances in our understanding of the effects of cervical hemisection (C2 SH) on diaphragm muscle (DIAm) EMG activity, very little is understood about the impact of C2 SH on the gamut of ventilatory and non-ventilatory transdiaphragmatic pressures (Pdi ). Recovery of DIAm activity following C2 SH is improved using a variety of approaches, but very few pharmaceuticals have been shown to be effective. One way of improving DIAm recovery is to enhance the amount of latent local spared connections onto phrenic motor neurons. A novel pegylated benzothiazole derivative enhances synaptogenesis in a variety of neurodegenerative conditions. Here, using a novel therapeutic SPG302, we show that 14 days of treatment with SPG302 ameliorated DIAm EMG and Pdi deficits compared with vehicle controls. Our results show that SPG302 is a compound with very promising potential for use in improving functional outcomes post-spinal cord injury.
Keywords: diaphragm muscle; electromyography; rehabilitation; spinal cord injury; transdiaphragmatic pressure.
© 2023 The Authors. The Journal of Physiology © 2023 The Physiological Society.
Conflict of interest statement
Figures







References
-
- Aubier M, Murciano D, Lecocguic Y, Viires N, and Pariente R (1985). Bilateral phrenic stimulation: a simple technique to assess diaphragmatic fatigue in humans. J Appl Physiol (1985) 58, 58–64. - PubMed
-
- Bellemare F, and Bigland-Ritchie B (1984). Assessment of human diaphragm strength and activation using phrenic nerve stimulation. Respir Physiol 58, 263–277. - PubMed
-
- Bellemare F, Bigland-Ritchie B, and Woods JJ (1986). Contractile properties of the human diaphragm in vivo. J Appl Physiol 61, 1153–1161. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous