

Smooth Muscle Mineralocorticoid Receptor Promotes Hypertension After Preeclampsia
- PMID: 36815487
- PMCID: PMC10119809
- DOI: 10.1161/CIRCRESAHA.122.321228
Smooth Muscle Mineralocorticoid Receptor Promotes Hypertension After Preeclampsia
Abstract
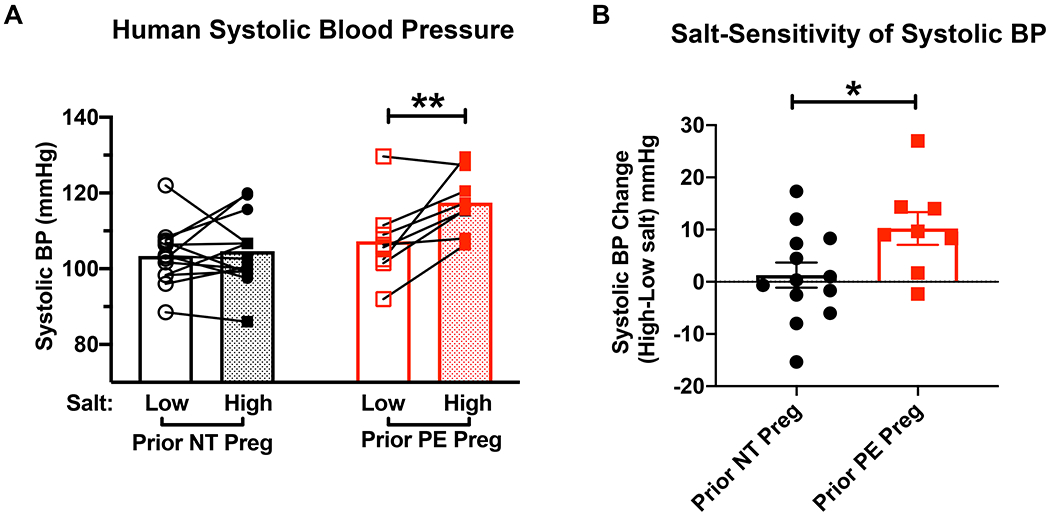
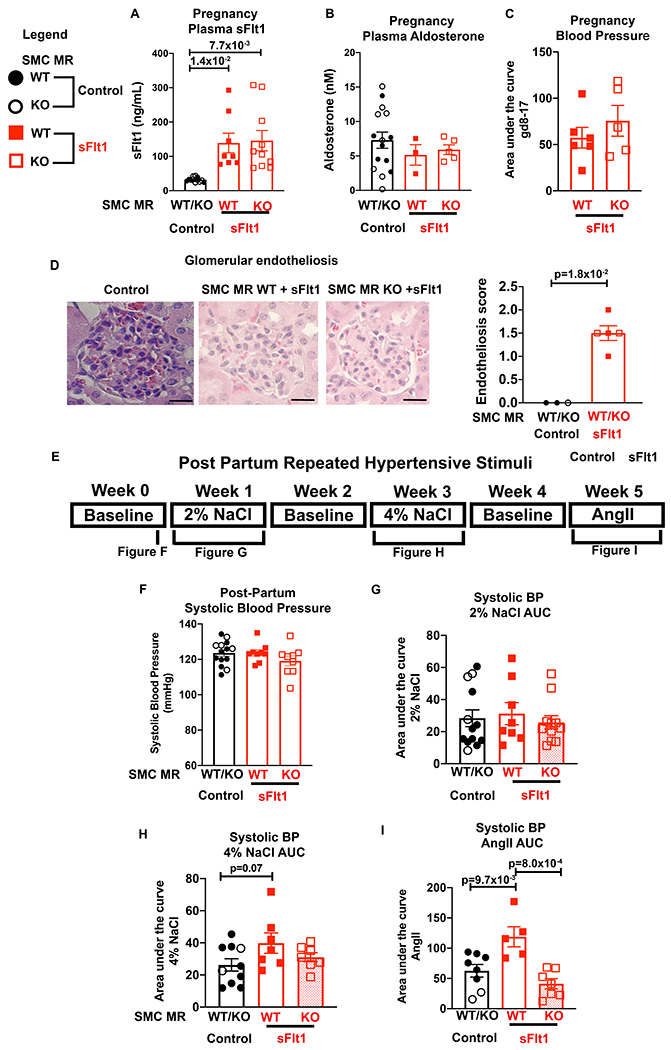
Background: Preeclampsia is a syndrome of high blood pressure (BP) with end organ damage in late pregnancy that is associated with high circulating soluble VEGF receptor (sFlt1 [soluble Fms-like tyrosine kinase 1]). Women exposed to preeclampsia have a substantially increased risk of hypertension after pregnancy, but the mechanism remains unknown, leaving a missed interventional opportunity. After preeclampsia, women have enhanced sensitivity to hypertensive stress. Since smooth muscle cell mineralocorticoid receptors (SMC-MR) are activated by hypertensive stimuli, we hypothesized that high sFlt1 exposure in pregnancy induces a postpartum state of enhanced SMC-MR responsiveness.
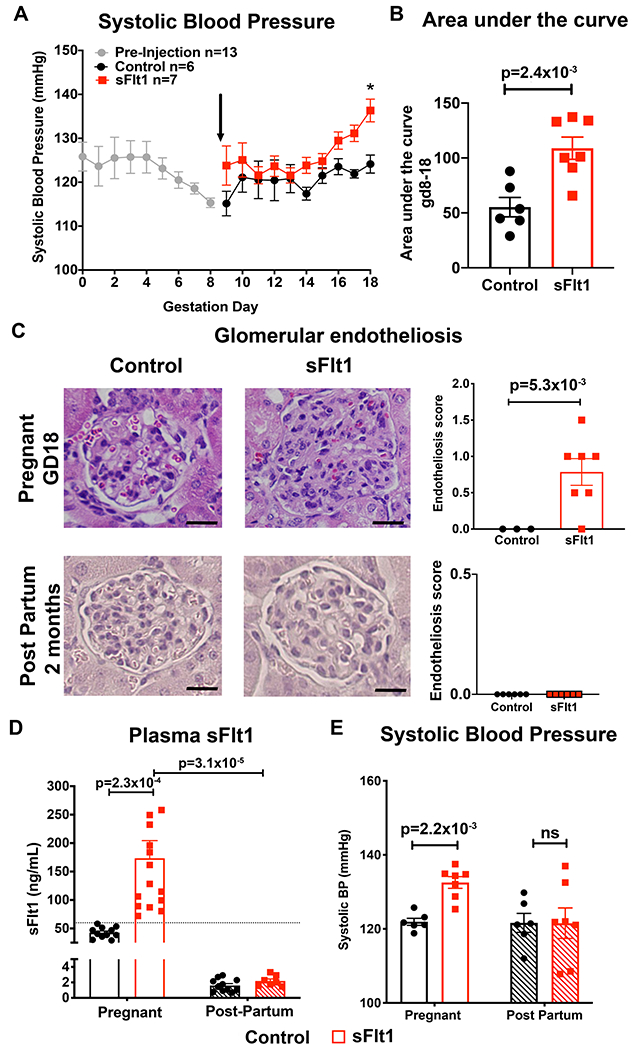
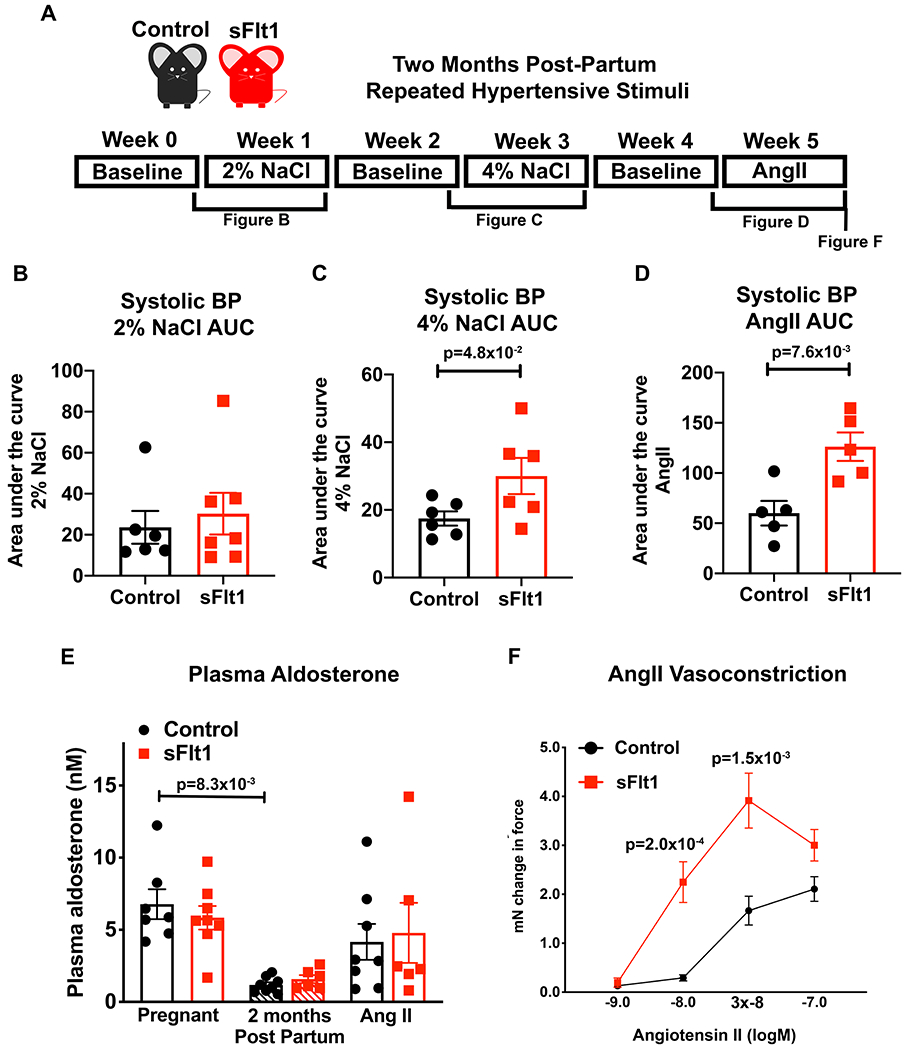
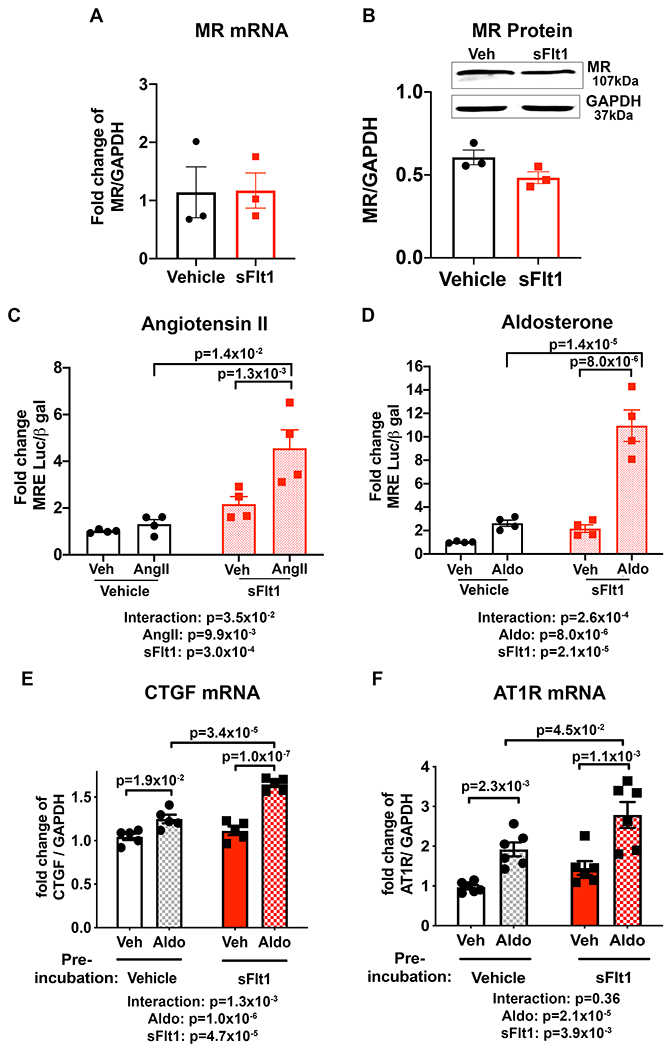
Methods: Postpartum BP response to high salt intake was studied in women with prior preeclampsia. MR transcriptional activity was assessed in vitro in sFlt1-treated SMC by reporter assays and PCR. Preeclampsia was modeled by transient sFlt1 expression in pregnant mice. Two months post-partum, mice were exposed to high salt and then to AngII (angiotensin II) and BP and vasoconstriction were measured.
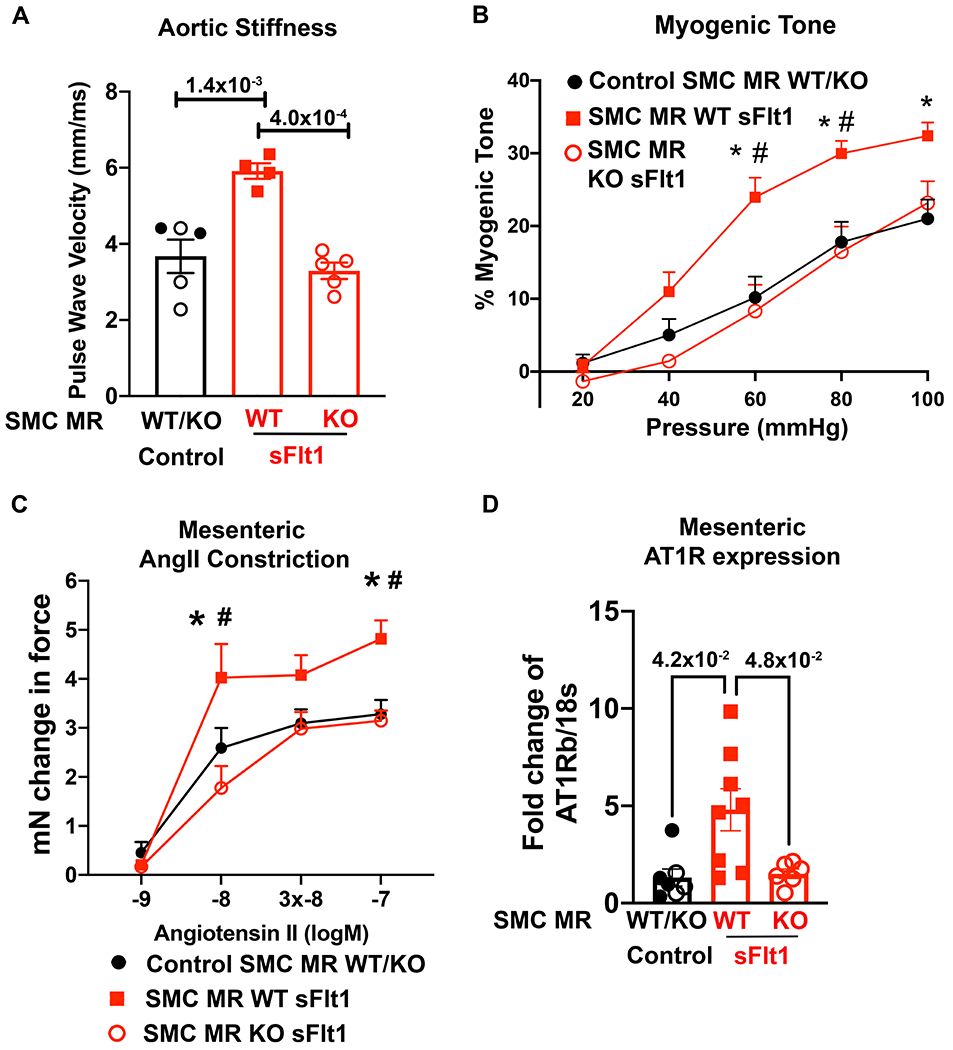
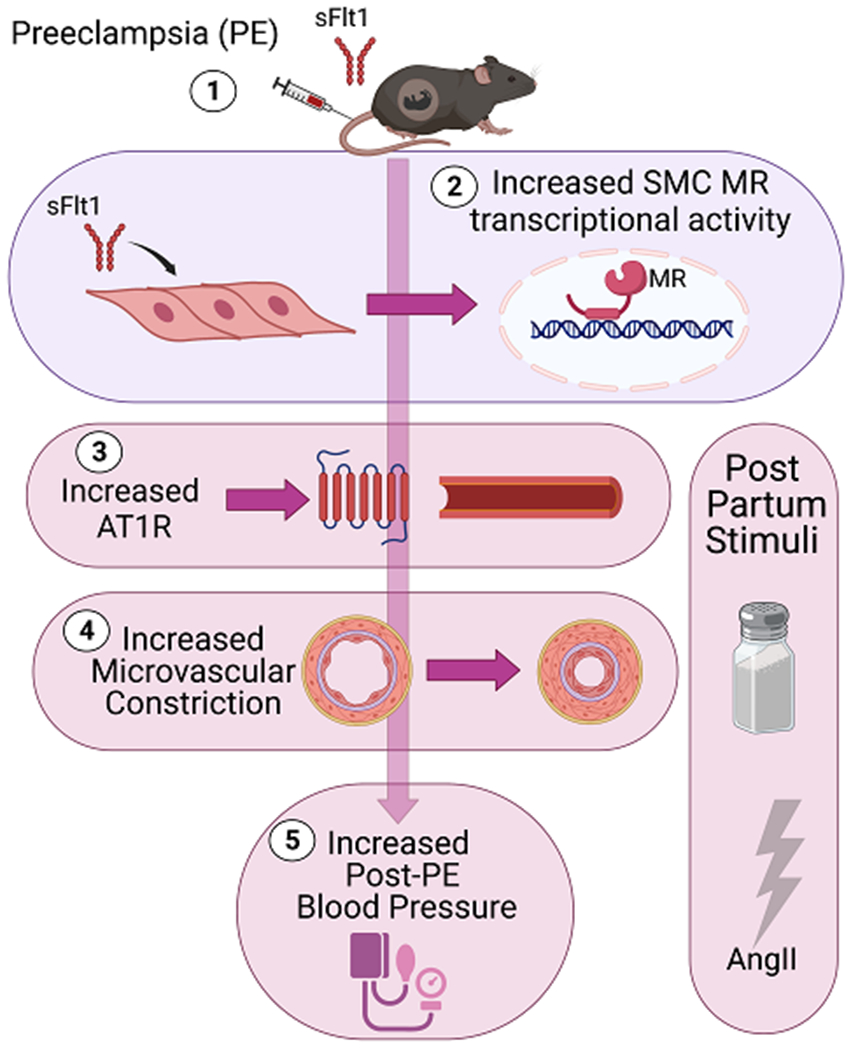
Results: Women exposed to preeclampsia had significantly enhanced salt sensitivity of BP verses those with a normotensive pregnancy. sFlt1 overexpression during pregnancy in mice induced elevated BP and glomerular endotheliosis, which resolved post-partum. The sFlt1 exposed post-partum mice had significantly increased BP response to 4% salt diet and to AngII infusion. In vitro, SMC-MR transcriptional activity in response to aldosterone or AngII was significantly increased after transient exposure to sFlt1 as was aldosterone-induced expression of AngII type 1 receptor. Post-partum, SMC-MR-KO mice were protected from the enhanced response to hypertensive stimuli after preeclampsia. Mechanistically, preeclampsia mice exposed to postpartum hypertensive stimuli develop enhanced aortic stiffness, microvascular myogenic tone, AngII constriction, and AngII type 1 receptor expression, all of which were prevented in SMC-MR-KO littermates.
Conclusions: These data support that sFlt1-induced vascular injury during preeclampsia produces a persistent state of enhanced sensitivity of SMC-MR to activation. This contributes to postpartum hypertension in response to common stresses and supports testing of MR antagonism to mitigate the increased cardiovascular risk in women after PE.
Keywords: angiotensin II; hypertension; mineralocorticoid receptor; myocytes, smooth muscle; pre-eclampsia.
Figures
References
-
- Chappell LC, Cluver CA, Kingdom J,Tong S. Pre-eclampsia. Lancet. 2021;398:341–354. - PubMed
-
- Ray JG, Vermeulen MJ, Schull MJ,Redelmeier DA. Cardiovascular health after maternal placental syndromes (CHAMPS): population-based retrospective cohort study. Lancet. 2005;366:1797–1803. - PubMed
-
- Tooher J, Thornton C, Makris A, Ogle R, Korda A,Hennessy A. All Hypertensive Disorders of Pregnancy Increase the Risk of Future Cardiovascular Disease. Hypertension. 2017;70:798–803. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
