

Predictors of residual low back pain in patients with osteoporotic vertebral fractures following percutaneous kyphoplasty
- PMID: 36816002
- PMCID: PMC9935818
- DOI: 10.3389/fsurg.2023.1119393
Predictors of residual low back pain in patients with osteoporotic vertebral fractures following percutaneous kyphoplasty
Abstract
Objective: Patients with osteoporotic vertebral fractures (OVFs) often suffer from residual low back pain (LBP) after percutaneous kyphoplasty (PKP). The purpose of this study was to identify risk factors for postoperative residual LBP and to develop a nomogram to predict the occurrence of residual LBP.
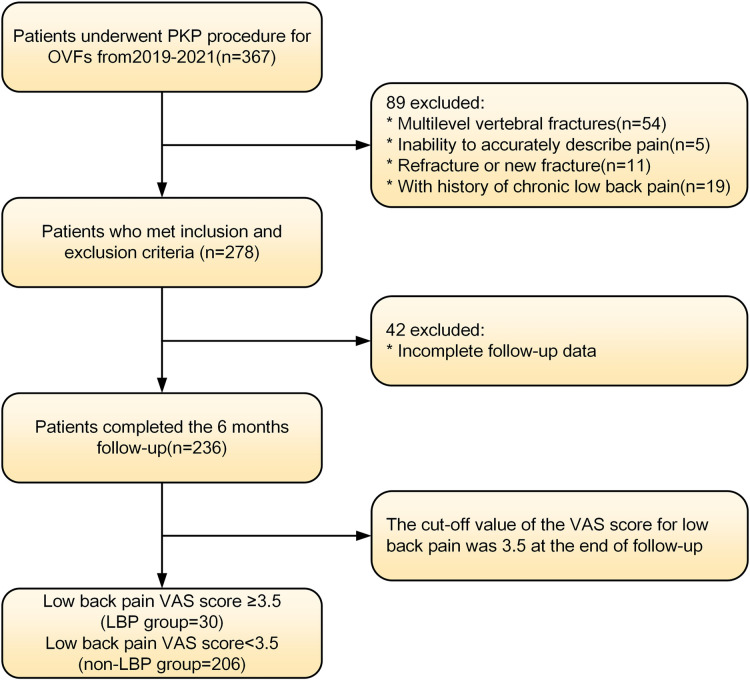
Methods: We retrospectively reviewed 236 patients who underwent PKP for OVFs and had a minimum follow-up of 12 months. The mean age was 72.1 ± 6.3, 74.3% were female and 25.7% were male. Patients with LBP VAS scores ≥ 3.5 at the 12th month postoperatively were considered to have residual LBP. Risk factors for residual LBP were identified by univariate and multifactorial logistic regression analysis. Then, a predictive nomogram was constructed and validated using the bootstrap method. The discrimination, calibration, and clinical utility of the nomogram were assessed using a receiver operating characteristic curve (ROC), a calibration curve, and a decision curve analysis (DCA).
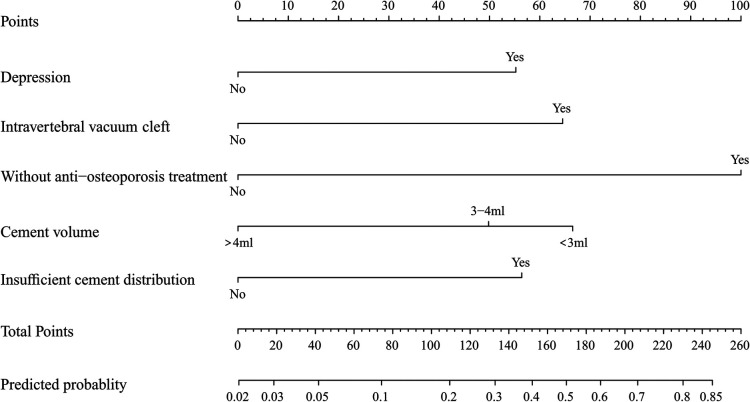
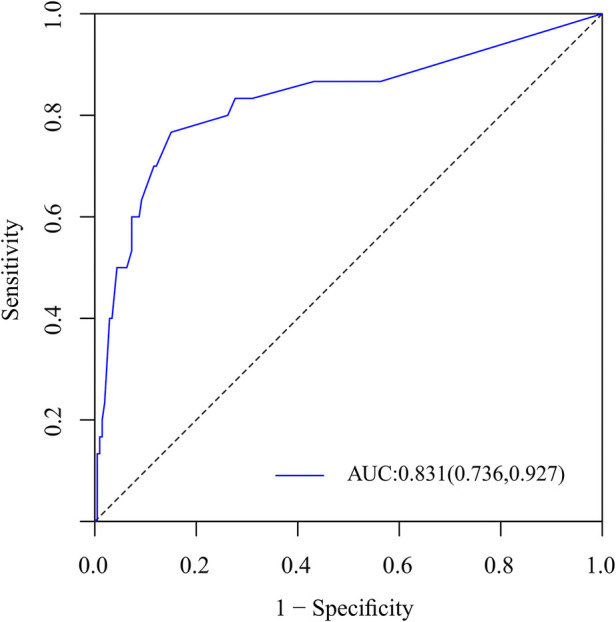
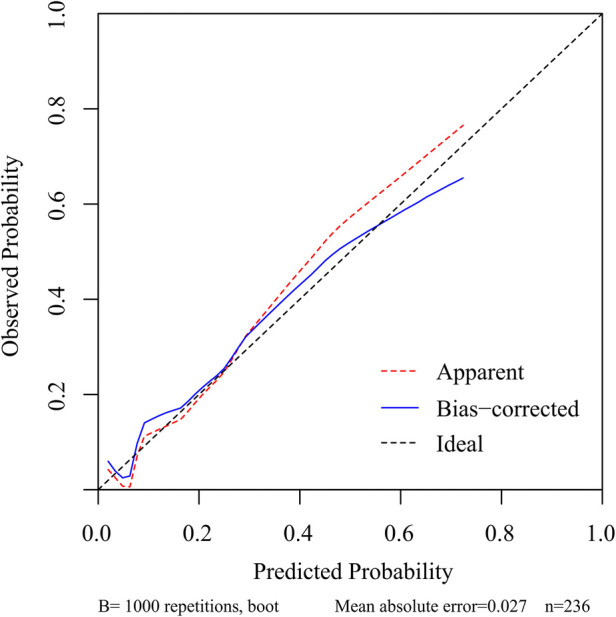
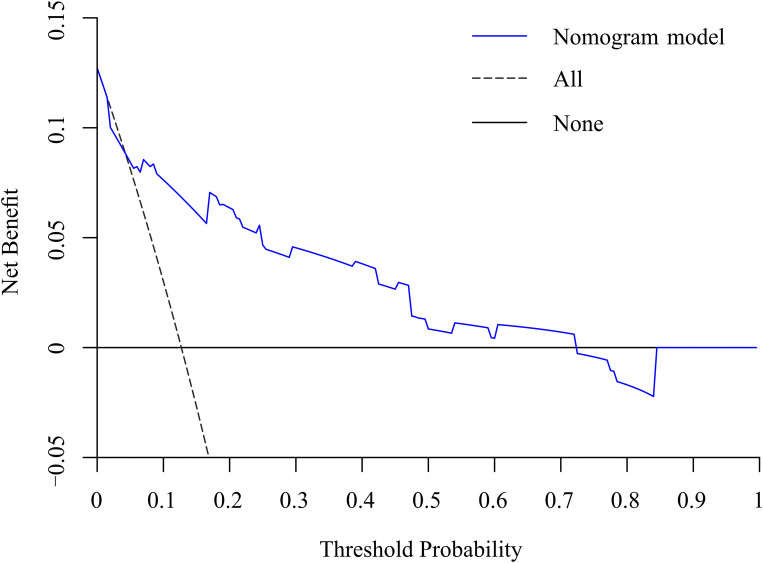
Results: univariate and multifactorial logistic regression analysis identified depression (P = 0.02), intravertebral vacuum cleft (P = 0.01), no anti-osteoporosis treatment (P < 0.001), cement volume <3 ml (P = 0.02), and cement distrubution (P = 0.01) as independent risk factors for residual LBP. The area under the ROC was 0.83 (0.74-0.93) and further validated by bootstrap method was 0.83 (0.73-0.92). The calibration curve illustrated the consistency between the predicted probability and the observed results. DCA showed that nomogram exhibits clinical utility and net benefit when the threshold probability is between 6% and 73%.
Conclusions: Our study found that depression, intravertebral vacuum cleft, no anti-osteoporosis treatment, cement volume <3 ml and cement distribution represent independent risk factors for residual LBP. The nomogram containing the above five predictors can accurately predict the risk of residual LBP after surgery.
Keywords: low back pain; nomogram; osteoporotic vertebral fractures; percutaneous kyphoplasty; risk factors.
© 2023 Yu, Luo, Wang, Yu, Sun and Tang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Establishment of a risk prediction model for residual low back pain in thoracolumbar osteoporotic vertebral compression fractures after percutaneous kyphoplasty.J Orthop Surg Res. 2024 Jan 6;19(1):41. doi: 10.1186/s13018-024-04528-y. J Orthop Surg Res. 2024. PMID: 38184651 Free PMC article.
-
A nomogram for predicting residual low back pain after percutaneous kyphoplasty in osteoporotic vertebral compression fractures.Osteoporos Int. 2023 Apr;34(4):749-762. doi: 10.1007/s00198-023-06681-2. Epub 2023 Feb 4. Osteoporos Int. 2023. PMID: 36738335
-
Risk factors for postoperative residual back pain after percutaneous kyphoplasty for osteoporotic vertebral compression fractures.Eur Spine J. 2020 Oct;29(10):2568-2575. doi: 10.1007/s00586-020-06493-6. Epub 2020 Jun 7. Eur Spine J. 2020. PMID: 32507918
-
Establishment and validation of a nomogram and web calculator for the risk of new vertebral compression fractures and cement leakage after percutaneous vertebroplasty in patients with osteoporotic vertebral compression fractures.Eur Spine J. 2022 May;31(5):1108-1121. doi: 10.1007/s00586-021-07064-z. Epub 2021 Nov 25. Eur Spine J. 2022. PMID: 34822018 Review.
-
Can Additional Facet Joint Block Improve the Clinical Outcome of Kyphoplasty for Acute Osteoporotic Vertebral Compression Fractures?Pain Physician. 2021 May;24(3):283-291. Pain Physician. 2021. PMID: 33988948
Cited by
-
Effect of thoracolumbar fascia injury on reported outcomes after percutaneous vertebroplasty.Front Surg. 2024 May 16;11:1379769. doi: 10.3389/fsurg.2024.1379769. eCollection 2024. Front Surg. 2024. PMID: 38817944 Free PMC article.
-
Incidence and predictors of residual back pain after percutaneous vertebral augmentation in osteoporotic vertebral compression fracture: a systematic review and meta analysis.Osteoporos Int. 2025 Jul 23. doi: 10.1007/s00198-025-07609-8. Online ahead of print. Osteoporos Int. 2025. PMID: 40699245 Review.
-
Incidence and prognostic factors of residual back pain in patients treated for osteoporotic vertebral compression fractures: a systematic review and meta-analysis.Eur Spine J. 2024 Dec;33(12):4521-4537. doi: 10.1007/s00586-024-08426-z. Epub 2024 Aug 6. Eur Spine J. 2024. PMID: 39103616
-
The Prevalence and Risk Factors of Residual Back Pain After Vertebroplasty for Osteoporotic Vertebral Compression Fractures: A Systematic Review and Meta-Analysis.Orthop Surg. 2025 Aug;17(8):2266-2280. doi: 10.1111/os.70095. Epub 2025 Jun 26. Orthop Surg. 2025. PMID: 40571423 Free PMC article. Review.
-
Association between vertebral bone quality score and residual back pain following percutaneous vertebroplasty for osteoporotic vertebral compression fractures.Eur Spine J. 2025 Feb;34(2):537-545. doi: 10.1007/s00586-024-08619-6. Epub 2024 Dec 17. Eur Spine J. 2025. PMID: 39688705
References
-
- Hinde K, Maingard J, Hirsch JA, Phan K, Asadi H, Chandra RV. Mortality outcomes of vertebral augmentation (vertebroplasty and/or balloon kyphoplasty) for osteoporotic vertebral compression fractures: a systematic review and meta-analysis. Radiology. (2020) 295(1):96–103. 10.1148/radiol.2020191294 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous