

Liver involvement in patients with COVID-19 infection: A comprehensive overview of diagnostic imaging features
- PMID: 36816623
- PMCID: PMC9932422
- DOI: 10.3748/wjg.v29.i5.834
Liver involvement in patients with COVID-19 infection: A comprehensive overview of diagnostic imaging features
Abstract
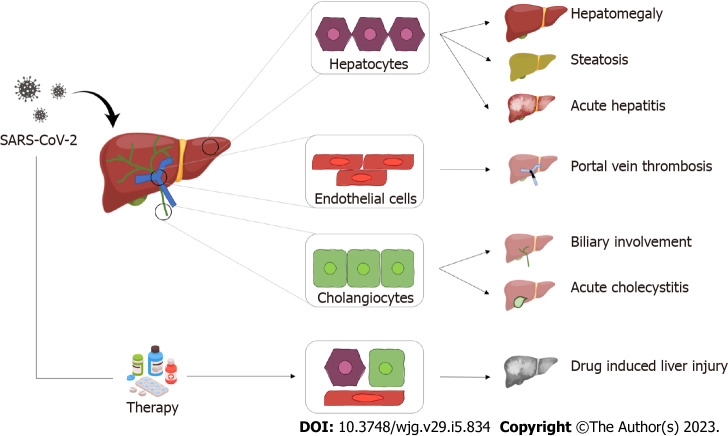
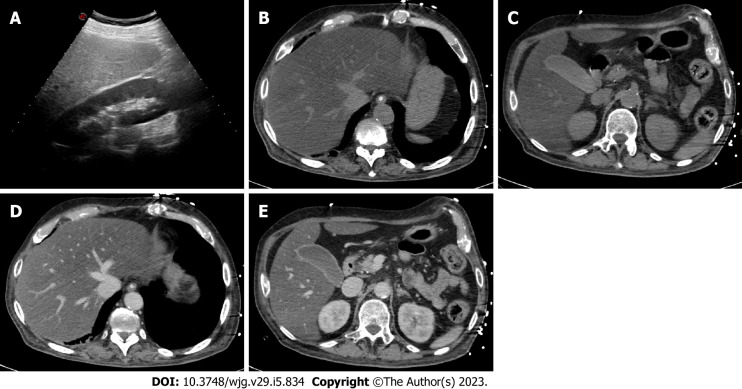
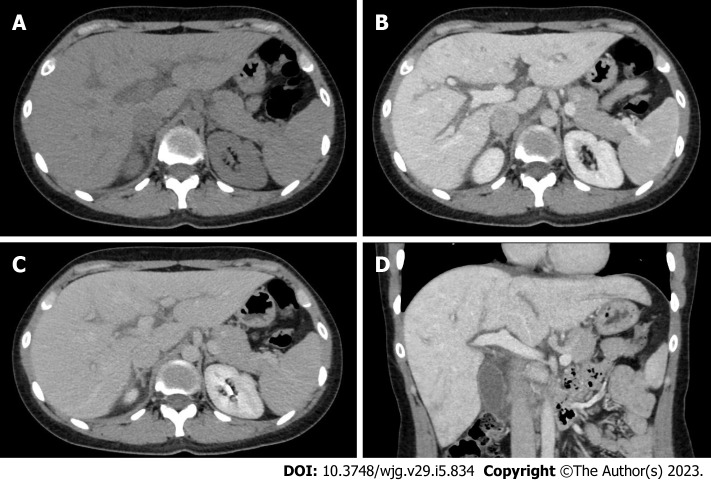
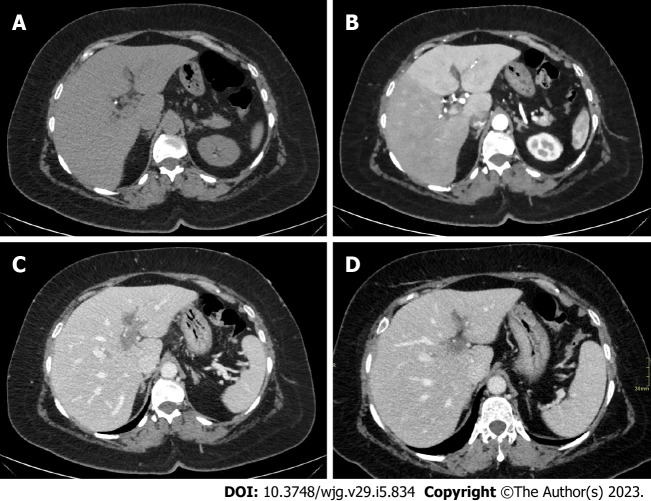
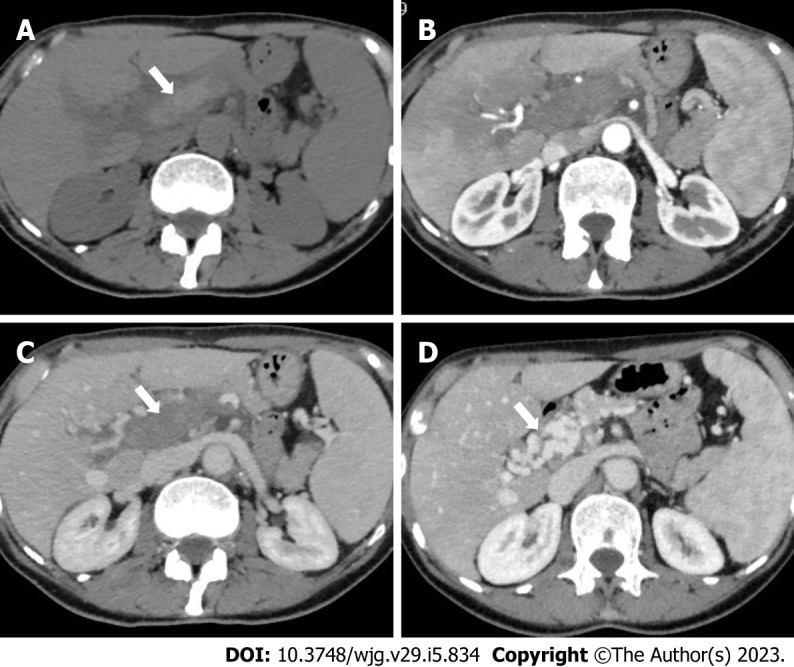
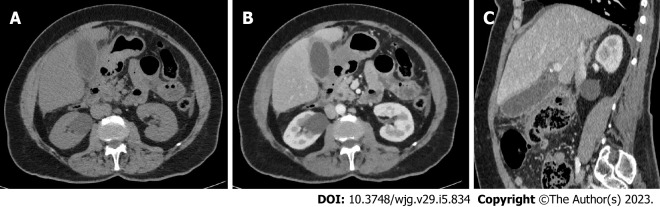
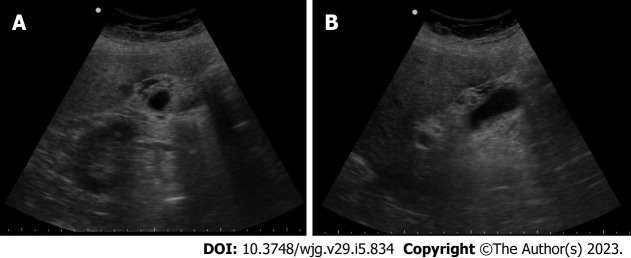
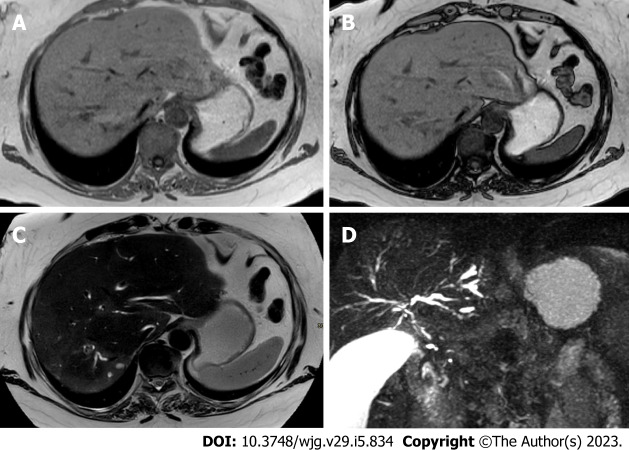
During the first wave of the pandemic, coronavirus disease 2019 (COVID-19) infection has been considered mainly as a pulmonary infection. However, different clinical and radiological manifestations were observed over time, including involvement of abdominal organs. Nowadays, the liver is considered one of the main affected abdominal organs. Hepatic involvement may be caused by either a direct damage by the virus or an indirect damage related to COVID-19 induced thrombosis or to the use of different drugs. After clinical assessment, radiology plays a key role in the evaluation of liver involvement. Ultrasonography (US), computed tomography (CT) and magnetic resonance imaging (MRI) may be used to evaluate liver involvement. US is widely available and it is considered the first-line technique to assess liver involvement in COVID-19 infection, in particular liver steatosis and portal-vein thrombosis. CT and MRI are used as second- and third-line techniques, respectively, considering their higher sensitivity and specificity compared to US for assessment of both parenchyma and vascularization. This review aims to the spectrum of COVID-19 liver involvement and the most common imaging features of COVID-19 liver damage.
Keywords: Adults; Biliary tract diseases; COVID-19; Fatty liver; Hepatic infarction; Hepatomegaly; Infection; Liver; Liver diseases; Liver failure; Magnetic resonance imaging; Pediatrics; SARS-CoV-2; Ultrasonography; X-Ray computed tomography.
©The Author(s) 2023. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures
References
-
- World Health Organization. Health Emergency Dashboard. [cited 7 September 2022]. Available from: https://score.tools.who.int/tools/survey-populations-and-health-risks/to...
-
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497–506. - PMC - PubMed
-
- Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Liu L, Shan H, Lei CL, Hui DSC, Du B, Li LJ, Zeng G, Yuen KY, Chen RC, Tang CL, Wang T, Chen PY, Xiang J, Li SY, Wang JL, Liang ZJ, Peng YX, Wei L, Liu Y, Hu YH, Peng P, Wang JM, Liu JY, Chen Z, Li G, Zheng ZJ, Qiu SQ, Luo J, Ye CJ, Zhu SY, Zhong NS China Medical Treatment Expert Group for Covid-19. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020;382:1708–1720. - PMC - PubMed
-
- Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A, Dequanter D, Blecic S, El Afia F, Distinguin L, Chekkoury-Idrissi Y, Hans S, Delgado IL, Calvo-Henriquez C, Lavigne P, Falanga C, Barillari MR, Cammaroto G, Khalife M, Leich P, Souchay C, Rossi C, Journe F, Hsieh J, Edjlali M, Carlier R, Ris L, Lovato A, De Filippis C, Coppee F, Fakhry N, Ayad T, Saussez S. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. 2020;277:2251–2261. - PMC - PubMed
-
- Cummings MJ, Baldwin MR, Abrams D, Jacobson SD, Meyer BJ, Balough EM, Aaron JG, Claassen J, Rabbani LE, Hastie J, Hochman BR, Salazar-Schicchi J, Yip NH, Brodie D, O'Donnell MR. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020;395:1763–1770. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
