

Different cytokine and chemokine profiles in hospitalized patients with COVID-19 during the first and second outbreaks from Argentina show no association with clinical comorbidities
- PMID: 36817433
- PMCID: PMC9929547
- DOI: 10.3389/fimmu.2023.1111797
Different cytokine and chemokine profiles in hospitalized patients with COVID-19 during the first and second outbreaks from Argentina show no association with clinical comorbidities
Abstract
Background: COVID-19 severity has been linked to an increased production of inflammatory mediators called "cytokine storm". Available data is mainly restricted to the first international outbreak and reports highly variable results. This study compares demographic and clinical features of patients with COVID-19 from Córdoba, Argentina, during the first two waves of the pandemic and analyzes association between comorbidities and disease outcome with the "cytokine storm", offering added value to the field.
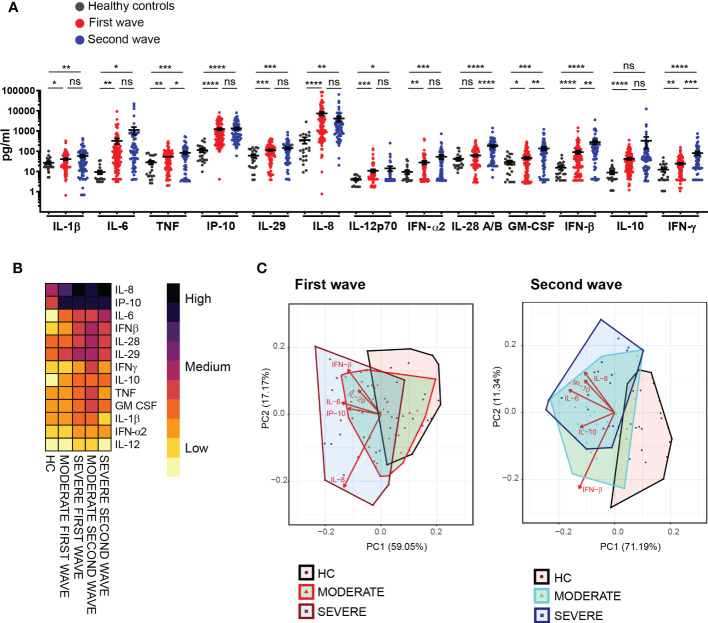
Methods: We investigated serum concentration of thirteen soluble mediators, including cytokines and chemokines, in hospitalized patients with moderate and severe COVID-19, without previous rheumatic and autoimmune diseases, from the central region of Argentina during the first and second infection waves. Samples from healthy controls were also assayed. Clinical and biochemical parameters were collected.
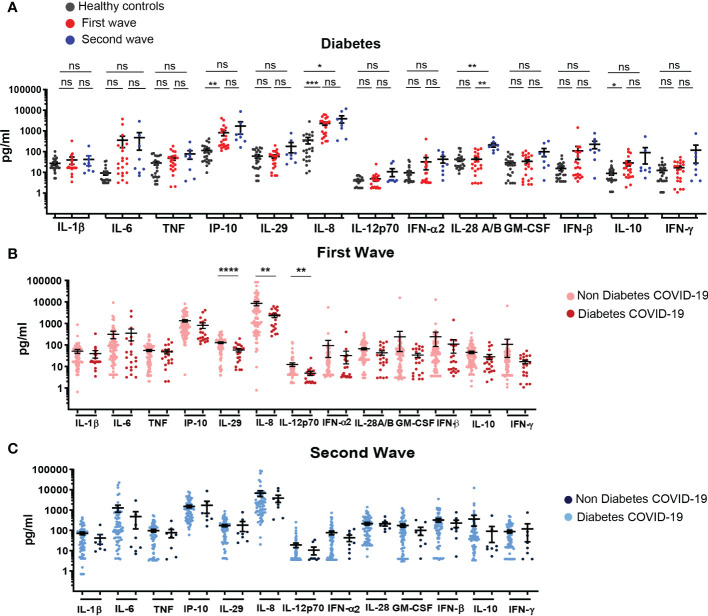
Results: Comparison between the two first COVID-19 waves in Argentina highlighted that patients recruited during the second wave were younger and showed less concurrent comorbidities than those from the first outbreak. We also recognized particularities in the signatures of systemic cytokines and chemokines in patients from both infection waves. We determined that concurrent pre-existing comorbidities did not have contribution to serum concentration of systemic cytokines and chemokines in COVID-19 patients. We also identified immunological and biochemical parameters associated to inflammation which can be used as prognostic markers. Thus, IL-6 concentration, C reactive protein level and platelet count allowed to discriminate between death and discharge in patients hospitalized with severe COVID-19 only during the first but not the second wave.
Conclusions: Our data provide information that deepens our understanding of COVID-19 pathogenesis linking demographic features of a COVID-19 cohort with cytokines and chemokines systemic concentration, presence of comorbidities and different disease outcomes. Altogether, our findings provide information not only at local level by delineating inflammatory/anti-inflammatory response of patients but also at international level addressing the impact of comorbidities and the infection wave in the variability of cytokine and chemokine production upon SARS-CoV-2 infection.
Keywords: COVID-19; SARS-CoV-2; comorbidities; cytokine storm; first infection wave; hypertension; mortality; second infection wave.
Copyright © 2023 Almada, Angiolini, Dho, Dutto, Gazzoni, Manzone-Rodríguez, Marín, Ponce, Arroyo, Quiróz, Iribarren, Cerbán, Morón, Amezcua Vesely, Cervi, Chiapello, Fozzatti, Icely, Maccioni, Montes, Motrán, Rodríguez-Galán, Stempin, Viano, Mena, Bertone, Abiega, Escudero, Kahn, Caeiro, Maletto, Acosta Rodríguez, Gruppi and Sotomayor.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Johns Hopkins Coronavirus Resource Center . Available at: https://coronavirus.jhu.edu/.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous