

Assessment of progesterone levels on the day of pregnancy test determination: A novel concept toward individualized luteal phase support
- PMID: 36817599
- PMCID: PMC9929287
- DOI: 10.3389/fendo.2023.1090105
Assessment of progesterone levels on the day of pregnancy test determination: A novel concept toward individualized luteal phase support
Abstract
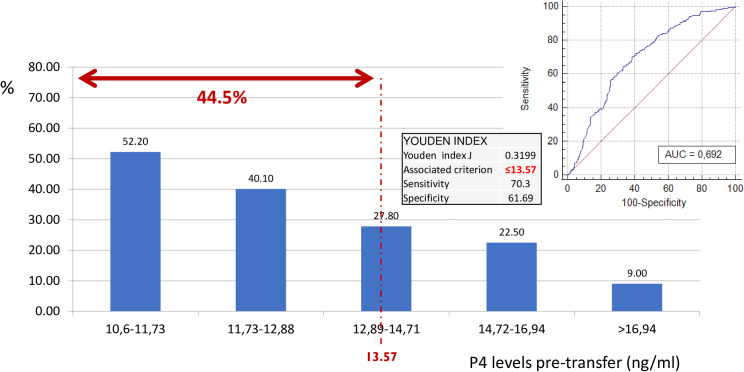
Research question: The main objective of the study is to define the optimal trade-off progesterone (P4) values on the day of embryo transfer (ET), to identify low P4-human chorionic gonadotropin (hCG), and to establish whether P4 supplementation started on the hCG day can increase the success rate of the frozen embryo transfer (FET) cycle.
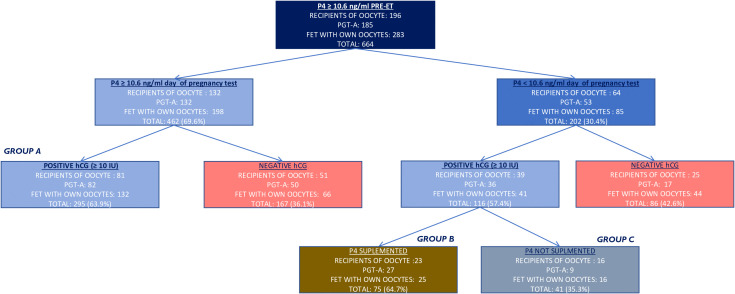
Design: A single-center, cohort, retrospective study with 664 hormone replacement therapy (HRT)-FET cycles analyzed female patients who received vaginal 600 mg/day of P4 starting from 6 days before the FET, had normal P4 values on the day before ET, and whose P4 on the day of the pregnancy test was assessed.
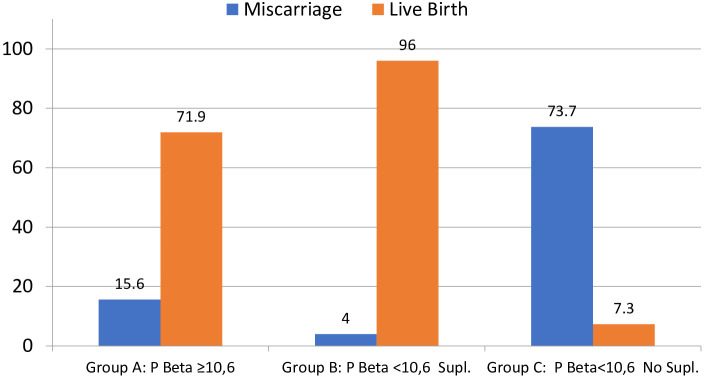
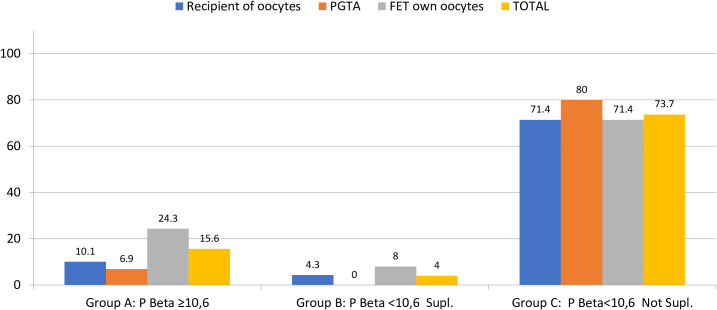
Results: Of the 664 cycles, 69.6% of cycles showed P4 ≥ 10.6 ng/ml, while 30.4% showed P4 < 10.6 ng/ml on the day of the hCG. Of the 411 chemical pregnancies detected, 71.8% had P4-hCG ≥ 10.6 ng/ml (group A), while 28.2% had P4-hCG < 10.6 ng/ml. Of the cycles with P4-hCG < 10.6 ng/ml, 64.7% (group B) were supplemented with a higher dose of vaginal P4 (1,000 mg/day), while 35.3% (group C) were maintained on the same dose of vaginal micronized P4. The live birth rate was 71.9%, 96%, and 7.3% for groups A, B, and C, respectively.
Conclusion: The likelihood to detect P4-hCG < 10.6 ng/ml decreased as the level of serum P4 the day before ET increased. The live birth rate (LBR) was shown to be significantly lower when P4 was low and not supplemented.
Keywords: artificially prepared endometrium; hCG and progesterone assessment; individualization of luteal phase; live birth rate; luteal phase support; progesterone supplementation.
Copyright © 2023 Racca, Alvarez, Garcia Martinez, Rodriguez, Gonzalez-Foruria, Polyzos and Coroleu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Rectal progesterone administration secures a high ongoing pregnancy rate in a personalized Hormone Replacement Therapy Frozen Embryo Transfer (HRT-FET) protocol: a prospective interventional study.Hum Reprod. 2023 Nov 2;38(11):2221-2229. doi: 10.1093/humrep/dead185. Hum Reprod. 2023. PMID: 37759346 Free PMC article.
-
Individualised luteal phase support in artificially prepared frozen embryo transfer cycles based on serum progesterone levels: a prospective cohort study.Hum Reprod. 2021 May 17;36(6):1552-1560. doi: 10.1093/humrep/deab031. Hum Reprod. 2021. PMID: 33686413
-
Comparison of Individualized Rescue Luteal Phase Support Strategies with Vaginal and Combined Vaginal & Subcutaneous Progesterone Administration in Artificial Frozen-Thawed Blastocyst Embryo Transfer Cycles Based on Serum Progesterone levels.Front Endocrinol (Lausanne). 2025 Jan 17;15:1503008. doi: 10.3389/fendo.2024.1503008. eCollection 2024. Front Endocrinol (Lausanne). 2025. PMID: 39897956 Free PMC article.
-
Individualized luteal phase support after fresh embryo transfer: unanswered questions, a review.Reprod Health. 2022 Jan 22;19(1):19. doi: 10.1186/s12978-021-01320-7. Reprod Health. 2022. PMID: 35065655 Free PMC article. Review.
-
Serum luteal phase progesterone in women undergoing frozen embryo transfer in assisted conception: a systematic review and meta-analysis.Fertil Steril. 2021 Dec;116(6):1534-1556. doi: 10.1016/j.fertnstert.2021.07.002. Epub 2021 Aug 10. Fertil Steril. 2021. PMID: 34384594
Cited by
-
Placental cell conditioned media modifies hematopoietic stem cell transcriptome invitro.Placenta. 2024 Jan;145:117-125. doi: 10.1016/j.placenta.2023.12.016. Epub 2023 Dec 15. Placenta. 2024. PMID: 38128222 Free PMC article.
References
-
- De Geyter C, Wyns C, Calhaz-Jorge C, de Mouzon J, Ferraretti AP, Kupka M, et al. . 20 years of the european IVF-monitoring consortium registry: What have we learned? a comparison with registries from two other regions. Hum Reprod (2020) 35 (12):2832–2849. doi: 10.1093/humrep/deaa250 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources