

Comparison of Single- and Multi-Echo Susceptibility-Weighted Imaging in Detecting Cerebral Arteriovenous Shunts: A Preliminary Study
- PMID: 36818708
- PMCID: PMC9935958
- DOI: 10.3348/jksr.2022.0080
Comparison of Single- and Multi-Echo Susceptibility-Weighted Imaging in Detecting Cerebral Arteriovenous Shunts: A Preliminary Study
Abstract
Purpose: To compare the sensitivities of T2-weighted image (T2WI) and susceptibility-weighted imaging (SWI) in detecting cerebral arteriovenous fistula (AVF), cerebral arteriovenous malformation (AVM), and carotid-cavernous sinus fistula (CCF), and to qualitatively evaluate single-echo SWI (s-SWI) and multi-echo SWI (m-SWI) in characterizing vascular lesions.
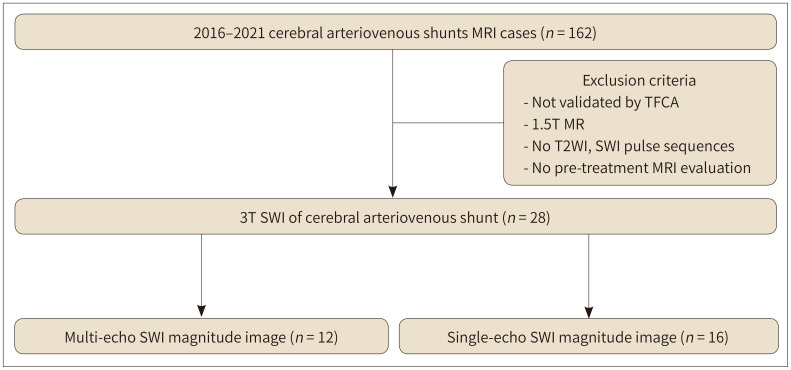
Materials and methods: From January 2016 to December 2021, cerebral angiography-proven lesions were recruited. The sensitivities of T2WI and SWI in detecting vascular lesions were compared using McNemar's test. Qualitative evaluations of s-SWI and m-SWI were categorized to be of poor, average, or good quality and compared using Fisher's exact test.
Results: A total of 24 patients (mean age: 61 years, 12 female, and 12 male) were enrolled. Twenty patients underwent s-SWI or m-SWI, and four patients underwent both. AVF, AVM, and CCF were diagnosed in 10, 11, and 3 patients, respectively. SWI demonstrated higher sensitivity compared to that of T2WI (82.1% vs. 53.6%, p = 0.013). m-SWI showed better image quality compared to that of s-SWI (good quality, 83.3% vs. 25.0%, p = 0.009).
Conclusion: SWI demonstrated a higher sensitivity for detecting cerebral arteriovenous shunts compared to that of T2WI. m-SWI exhibited better image quality compared to that of s-SWI in characterizing vascular lesions.
목적: 뇌동정맥루(arteriovenous fistula; 이하 AVF), 뇌동정맥기형(arteriovenous malformation; 이하 AVM), 경동맥해면정맥동루(carotid-cavernous sinus fistula; 이하 CCF) 등 뇌동정맥단락을 진단하는 데 있어서, T2 강조영상(T2-weighted imaging; 이하 T2WI)과 자화율 강조영상(susceptibility-weighted imaging; 이하 SWI)의 민감도를 비교하고, 단일 에코(single-echo) SWI(이하 s-SWI)와 다중 에코(multi-echo) SWI (이하 m-SWI)의 전반적인 영상 질을 비교하고자 하였다.
대상과 방법: 2016년부터 2021년까지 뇌혈관조영술로 입증된 뇌동정맥단락을 조사하였다. 뇌동정맥단락에 대한 T2WI와 SWI의 민감도를 McNemar’s Test를 이용하여 비교하였다. s-SWI와 m-SWI의 영상 질을 나쁨, 보통, 좋음으로 분류하고 Fisher’s exact test를 이용하여 그 비율을 비교하였다.
결과: 총 24명의 환자(중위 연령: 61세, 여성: 12명, 남성: 12명)가 연구에 포함되었다. 그중 4명은 s-SWI와 m-SWI 두 가지의 SWI로, 나머지 20명은 이 중 한 가지의 SWI로 검사하였다. 10명은 AVF, 11명은 AVM, 3명은 CCF로 진단되었고, 이와 같은 뇌동정맥단락에 대해, SWI는 T2WI 보다 유의하게 높은 민감도를 보였다(82.1% vs. 53.6%, p = 0.013). m-SWI는 s-SWI 보다 좋은 영상 질의 비율이 유의하게 높았다(83.3% vs. 25.0%, p = 0.009).
결론: SWI는 T2WI 보다 뇌동정맥단락을 더 민감하게 진단해 낼 수 있었으며, m-SWI는 s-SWI보다 혈관질환을 평가하는데 더 좋은 영상 질을 보였다.
Keywords: Angiography; Arteriovenous Fistula; Arteriovenous Malformation; Carotid-Cavernous Sinus Fistula; Magnetic Resonance Imaging.
Copyrights © 2023 The Korean Society of Radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
Figures



Similar articles
-
Accuracy of SWI sequences compared to T2*-weighted gradient echo sequences in the detection of cerebral cavernous malformations in the familial form.Neuroradiol J. 2016 Oct;29(5):326-35. doi: 10.1177/1971400916665376. Epub 2016 Aug 22. Neuroradiol J. 2016. PMID: 27549150 Free PMC article.
-
Susceptibility-weighted imaging for the evaluation of patients with familial cerebral cavernous malformations: a comparison with t2-weighted fast spin-echo and gradient-echo sequences.AJNR Am J Neuroradiol. 2008 Jan;29(1):154-8. doi: 10.3174/ajnr.A0748. Epub 2007 Oct 18. AJNR Am J Neuroradiol. 2008. PMID: 17947370 Free PMC article.
-
The value of susceptibility weighted magnetic resonance imaging in evaluation of patients with familial cerebral cavernous angioma.Int J Clin Exp Med. 2014 Dec 15;7(12):5296-302. eCollection 2014. Int J Clin Exp Med. 2014. PMID: 25664034 Free PMC article.
-
Magnetic resonance susceptibility weighted imaging in neurosurgery: current applications and future perspectives.J Neurosurg. 2015 Dec;123(6):1463-75. doi: 10.3171/2015.1.JNS142349. Epub 2015 Jul 24. J Neurosurg. 2015. PMID: 26207600 Review.
-
[Diagnostic imaging of hemangiomas in the brain].Brain Nerve. 2011 Jan;63(1):5-15. Brain Nerve. 2011. PMID: 21228443 Review. Japanese.
References
-
- Abecassis IJ, Xu DS, Batjer HH, Bendok BR. Natural history of brain arteriovenous malformations: a systematic review. Neurosurg Focus. 2014;37:E7 - PubMed
-
- Ellis JA, Goldstein H, Connolly ES, Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32:E9 - PubMed
-
- Hillman J. Population-based analysis of arteriovenous malformation treatment. J Neurosurg. 2001;95:633–637. - PubMed
LinkOut - more resources
Full Text Sources
