

Varied Presentation of Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy (ARVD/C): A Case Series
- PMID: 36819412
- PMCID: PMC9934937
- DOI: 10.7759/cureus.33883
Varied Presentation of Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy (ARVD/C): A Case Series
Abstract
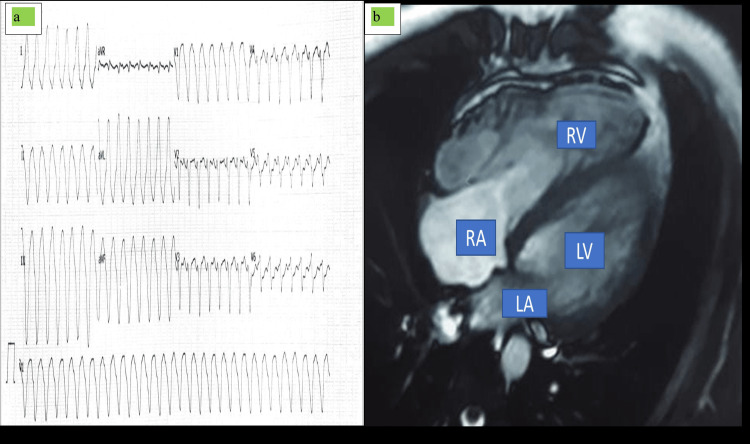
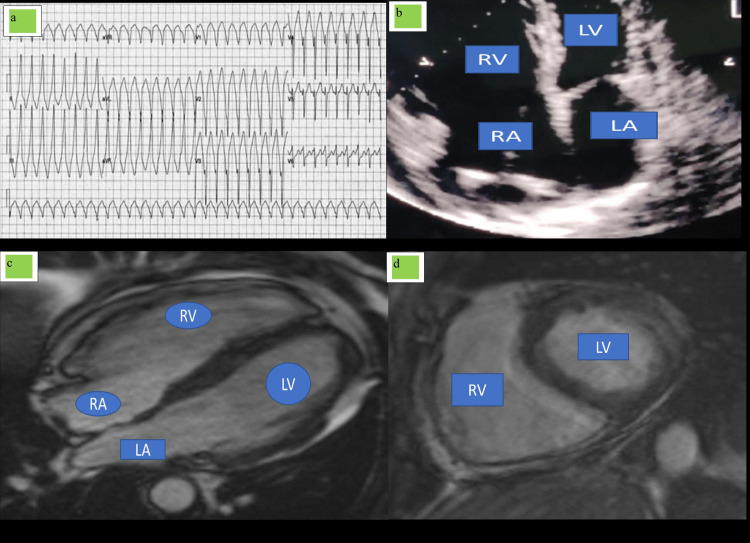
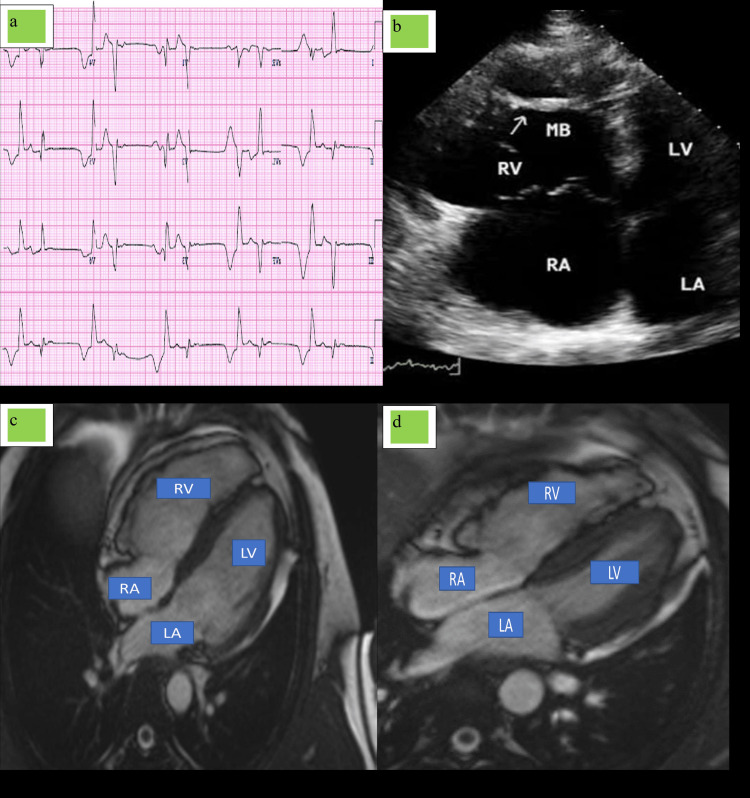
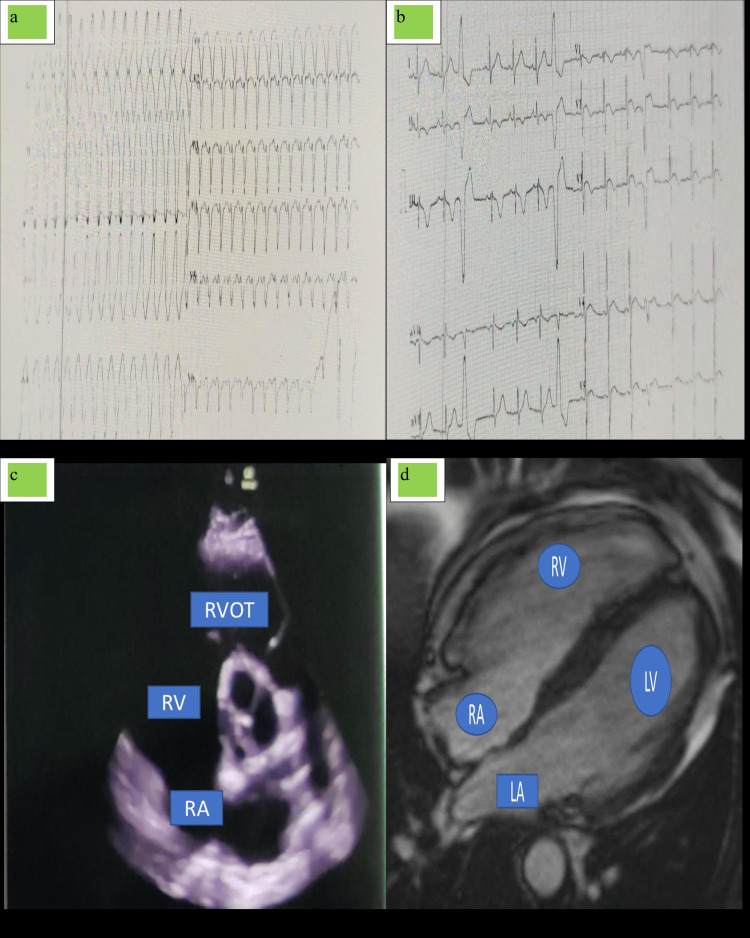
Arrhythmogenic right ventricular dysplasia (ARVD) is a genetically predisposed form of cardiomyopathy that mainly affects young individuals resulting in fatal ventricular arrhythmias leading to sudden cardiac death. ARVD has 50% of cases that involve both the right ventricle (RV) and left ventricle (LV), but only a small number of cases involve an isolated left ventricle. In this case series, five patients (four males and one female) with a diagnosis of ARVD presented to our center with varied clinical presentations across a wide range of age groups. The MRI of all five cases showed dilated right atrium (RA)/RV with right ventricular free wall dyskinesia. Two-dimensional (2D) MRI showed aneurysmal outpouching with diffuse free wall enhancement. Automated implantable cardioverter defibrillator (AICD) was implanted uneventfully in all five patients, and the patients were discharged with oral medications such as low-dose diuretics, beta-blockers, spironolactone, angiotensin-converting enzymes (ACE) inhibitors, amiodarone, and anxiolytics. Until now, the patients were doing well on follow-up visits. The therapeutic management of patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) has evolved over the years and continues to be an important challenge. To further improve risk stratification and treatment of patients, more information is needed on natural history, long-term prognosis, and risk assessment. Special attention should be focused on the identification of patients who would benefit from implantable cardioverter-defibrillator (ICD) implantation in comparison to pharmacological and other nonpharmacological approaches.
Keywords: arvd; cardiomyopathy; right bundle branch block; right ventricle; ventricular tachycardia.
Copyright © 2023, Mishra et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Implantable cardioverter defibrillators in arrhythmogenic right ventricular dysplasia/cardiomyopathy: patient outcomes, incidence of appropriate and inappropriate interventions, and complications.Circ Arrhythm Electrophysiol. 2013 Jun;6(3):562-8. doi: 10.1161/CIRCEP.113.000392. Epub 2013 May 14. Circ Arrhythm Electrophysiol. 2013. PMID: 23673907 Review.
-
Arrhythmogenic right ventricular dysplasia/cardiomyopathy.Curr Treat Options Cardiovasc Med. 2005 Dec;7(6):467-75. doi: 10.1007/s11936-005-0032-0. Curr Treat Options Cardiovasc Med. 2005. PMID: 16283974
-
Prevalence of atrial arrhythmias in arrhythmogenic right ventricular dysplasia/cardiomyopathy.Heart Rhythm. 2013 Nov;10(11):1661-8. doi: 10.1016/j.hrthm.2013.08.032. Epub 2013 Aug 28. Heart Rhythm. 2013. PMID: 23994726
-
Symptomatic arrhythmogenic right ventricular dysplasia/cardiomyopathy. A two-centre retrospective study of 15 symptomatic ARVD/C cases and focus on the diagnostic value of MRI in symptomatic ARVD/C patients.Acta Cardiol. 2008 Apr;63(2):181-9. doi: 10.2143/AC.63.2.2029526. Acta Cardiol. 2008. PMID: 18468198
-
Current and state of the art on the electrophysiologic characteristics and catheter ablation of arrhythmogenic right ventricular dysplasia/cardiomyopathy.J Cardiol. 2015 Jun;65(6):441-50. doi: 10.1016/j.jjcc.2014.12.023. Epub 2015 Mar 25. J Cardiol. 2015. PMID: 25818480 Review.
References
-
- Arrhythmogenic right ventricular cardiomyopathy: progress toward personalized management. James CA, Calkins H. Annu Rev Med. 2019;70:1–18. - PubMed
-
- Arrhythmogenic right ventricular dysplasia/cardiomyopathy: need for an international registry. Study Group on Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy of the Working Groups on Myocardial and Pericardial Disease and Arrhythmias of the European Society of Cardiology and of the Scientific Council on Cardiomyopathies of the World Heart Federation. Corrado D, Fontaine G, Marcus FI, McKenna WJ, Nava A, Thiene G, Wichter T. Circulation. 2000;101:0–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous