

EML4-ALK rearrangement of lung large cell neuroendocrine carcinoma: a case report
- PMID: 36819595
- PMCID: PMC9929752
- DOI: 10.21037/atm-22-6062
EML4-ALK rearrangement of lung large cell neuroendocrine carcinoma: a case report
Abstract
Background: Lung large cell neuroendocrine carcinoma (L-LCNEC) is a subtype of lung cancer with a low incidence and a high degree of malignancy. For early stage patients, surgical treatment is limited, and the risk of postoperative recurrence is high. For patients with unresectable or advanced disease, platinum-based chemotherapy is currently the mainstay of treatment, but its efficacy is unsatisfactory. L-LCNEC with the anaplastic lymphoma kinase (ALK) gene mutation is very rare and currently has no standard therapy. In this article, we report the case of a locally advanced L-LCNEC patient with ALK mutations who underwent first-line treatment with alectinib.
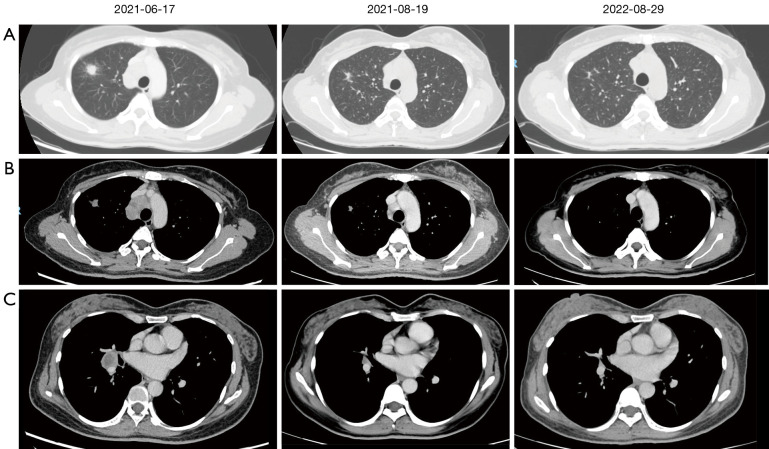
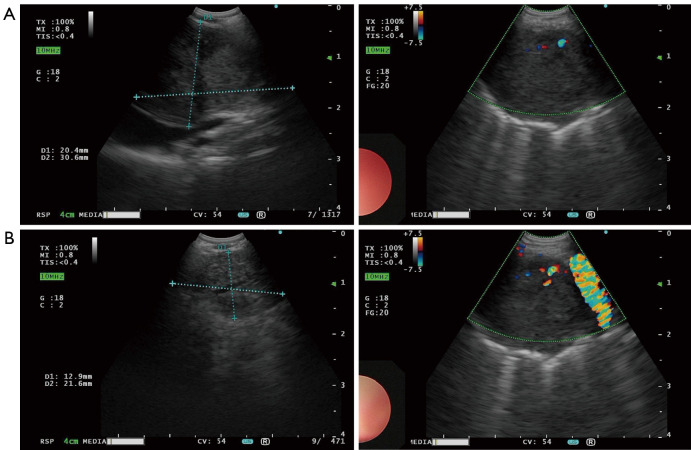
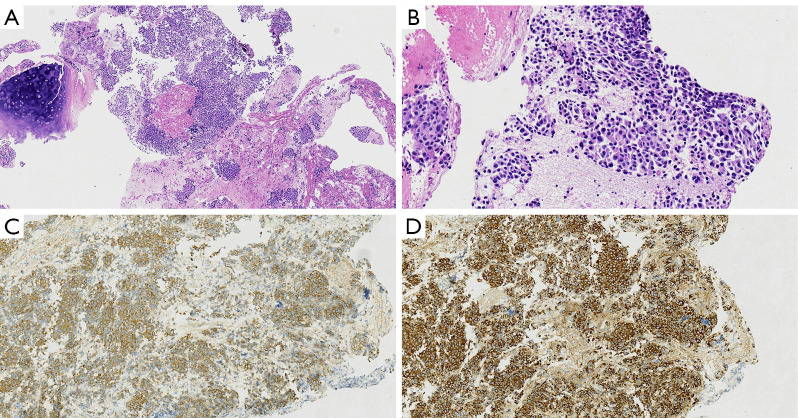
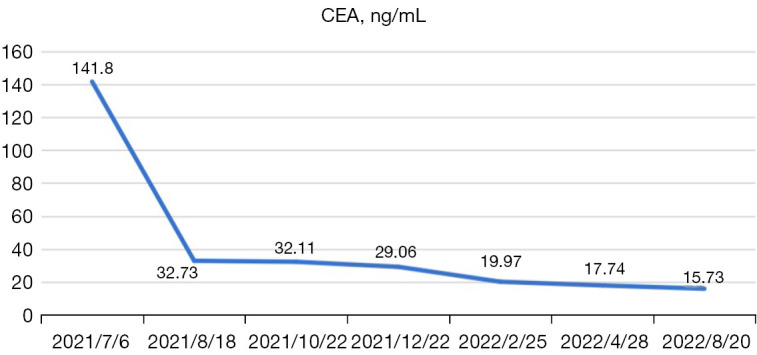
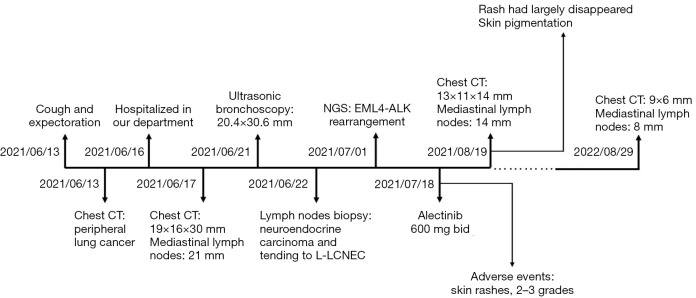
Case description: A previously healthy, 46-year-old, non-smoking woman was clinically diagnosed with unresectable locally advanced L-LCNEC. Next generation sequencing (NGS) of the patient's plasma and tumor specimen showed echinoderm microtubule-associated protein-like 4 (EML-4) (exon 13)-ALK (exon 20) fusion with a mutation frequency of 14.48% and 15.37%. The patient refused chemotherapy, and received first-line treatment with alectinib 600 mg, bis in die (bid), per day. After taking alectinib for 1 month, the patient's chest enhanced computed tomography (CT) scan showed a partial response (PR). After 12 months of treatment with alectinib, a radiological evaluation showed that the patient had maintained the PR. A grade 2-3 rash was observed at the beginning of the treatment. After symptomatic treatment, the rash disappeared, and the side effects were fully tolerated. At present, the patient can work normally, has a performance status of 0 and has not experience any major adverse events.
Conclusions: Our case suggests that the first-line use of targeted therapy is also a good choice for L-LCNEC patients of stage III with gene mutations. The side effects are light, the patient can tolerate well, and the quality of life of can be improved.
Keywords: Alectinib; Lung large cell neuroendocrine carcinoma (L-LCNEC); anaplastic lymphoma kinase (ALK); case report; neuroendocrine tumors (NET).
2023 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-6062/coif). The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Dramatic response to alectinib in an ALK-positive LCNEC patient with a poor performance status: A case report.Respirol Case Rep. 2021 Aug 3;9(9):e0817. doi: 10.1002/rcr2.817. eCollection 2021 Sep. Respirol Case Rep. 2021. PMID: 34377493 Free PMC article.
-
Two case reports: EML4-ALK rearrangement large cell neuroendocrine carcinoma and literature review.Front Oncol. 2023 Nov 1;13:1227980. doi: 10.3389/fonc.2023.1227980. eCollection 2023. Front Oncol. 2023. PMID: 38023218 Free PMC article.
-
Lung adenocarcinoma harboring complex EML4-ALK fusion and BRAF V600E co-mutation responded to alectinib.Medicine (Baltimore). 2022 Oct 7;101(40):e30913. doi: 10.1097/MD.0000000000030913. Medicine (Baltimore). 2022. PMID: 36221356 Free PMC article.
-
Coexistence of a novel NBEA-ALK, EML4-ALK double-fusion in a lung adenocarcinoma patient and response to alectinib: A case report.Lung Cancer. 2021 Dec;162:86-89. doi: 10.1016/j.lungcan.2021.10.015. Epub 2021 Nov 5. Lung Cancer. 2021. PMID: 34763158 Review.
-
Anaplastic lymphoma kinase rearrangement in lung cancer: its biological and clinical significance.Respir Investig. 2014 Nov;52(6):330-8. doi: 10.1016/j.resinv.2014.06.005. Epub 2014 Jul 30. Respir Investig. 2014. PMID: 25453376 Review.
Cited by
-
A rare case report of a primary lung cancer comprising adenocarcinoma and atypical carcinoid tumor, with the carcinoid component harboring EML4-ALK rearrangement.Transl Lung Cancer Res. 2024 May 31;13(5):1150-1162. doi: 10.21037/tlcr-24-352. Epub 2024 May 24. Transl Lung Cancer Res. 2024. PMID: 38854939 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous