

Sources of exposure and risk among employees infected with severe acute respiratory coronavirus virus 2 (SARS-CoV-2) in a large, urban, tertiary-care hospital in the United States
- PMID: 36819772
- PMCID: PMC9936511
- DOI: 10.1017/ash.2022.366
Sources of exposure and risk among employees infected with severe acute respiratory coronavirus virus 2 (SARS-CoV-2) in a large, urban, tertiary-care hospital in the United States
Abstract
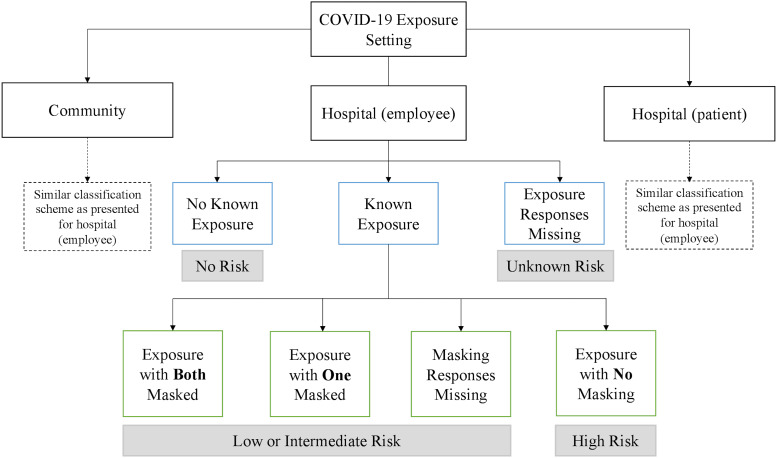
Objective: Hospital employees are at risk of SARS-CoV-2 infection through transmission in 3 settings: (1) the community, (2) within the hospital from patient care, and (3) within the hospital from other employees. We evaluated probable sources of infection among hospital employees based on reported exposures before infection.
Design: A structured survey was distributed to participants to evaluate presumed COVID-19 exposures (ie, close contacts with people with known or probable COVID-19) and mask usage. Participants were stratified into high, medium, low, and unknown risk categories based on exposure characteristics and personal protective equipment.
Setting: Tertiary-care hospital in Boston, Massachusetts.
Participants: Hospital employees with a positive SARS-CoV-2 PCR test result between March 2020 and January 2021. During this period, 573 employees tested positive, of whom 187 (31.5%) participated.
Results: We did not detect a statistically significant difference in the proportion of employees who reported any exposure (ie, close contacts at any risk level) in the community compared with any exposure in the hospital, from either patients or employees. In total, 131 participants (70.0%) reported no known high-risk exposure (ie, unmasked close contacts) in any setting. Among those who could identify a high-risk exposure, employees were more likely to have had a high-risk exposure in the community than in both hospital settings combined (odds ratio, 1.89; P = .03).
Conclusions: Hospital employees experienced exposure risks in both community and hospital settings. Most employees were unable to identify high-risk exposures prior to infection. When respondents identified high-risk exposures, they were more likely to have occurred in the community.
© The Author(s) 2023.
Figures
Similar articles
-
Perceptions of sources of transmission among hospital employees infected with severe acute respiratory coronavirus 2 (SARS-CoV-2) in an urban tertiary care hospital: a qualitative study to inform future pandemic management.Antimicrob Steward Healthc Epidemiol. 2025 Mar 14;5(1):e78. doi: 10.1017/ash.2025.39. eCollection 2025. Antimicrob Steward Healthc Epidemiol. 2025. PMID: 40109910 Free PMC article.
-
Efficacy of hydroxychloroquine for post-exposure prophylaxis to prevent severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among adults exposed to coronavirus disease (COVID-19): a structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Jun 3;21(1):475. doi: 10.1186/s13063-020-04446-4. Trials. 2020. PMID: 32493478 Free PMC article.
-
Quantification of Occupational and Community Risk Factors for SARS-CoV-2 Seropositivity Among Health Care Workers in a Large U.S. Health Care System.Ann Intern Med. 2021 May;174(5):649-654. doi: 10.7326/M20-7145. Epub 2021 Jan 29. Ann Intern Med. 2021. PMID: 33513035 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
Masks for Prevention of Respiratory Virus Infections, Including SARS-CoV-2, in Health Care and Community Settings : A Living Rapid Review.Ann Intern Med. 2020 Oct 6;173(7):542-555. doi: 10.7326/M20-3213. Epub 2020 Jun 24. Ann Intern Med. 2020. Update in: Ann Intern Med. 2023 Jun;176(6):827-835. doi: 10.7326/M23-0570. PMID: 32579379 Free PMC article. Updated. Review.
Cited by
-
Perceptions of sources of transmission among hospital employees infected with severe acute respiratory coronavirus 2 (SARS-CoV-2) in an urban tertiary care hospital: a qualitative study to inform future pandemic management.Antimicrob Steward Healthc Epidemiol. 2025 Mar 14;5(1):e78. doi: 10.1017/ash.2025.39. eCollection 2025. Antimicrob Steward Healthc Epidemiol. 2025. PMID: 40109910 Free PMC article.
References
-
- WHO Director-General’s opening remarks at the media briefing on COVID-19. World Health Organization website. https://www.who.int/director-general/speeches/detail/who-director-genera.... Published March 11, 2020. Accessed October 31, 2021.
-
- Shortage of personal protective equipment endangering health workers worldwide. World Health Organization website. https://www.who.int/news/item/03-03-2020-shortage-of-personal-protective.... Published March 3, 2020. Accessed October 31, 2021.
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous