

Characteristics and risk factors for post-COVID-19 breathlessness after hospitalisation for COVID-19
- PMID: 36820079
- PMCID: PMC9790090
- DOI: 10.1183/23120541.00274-2022
Characteristics and risk factors for post-COVID-19 breathlessness after hospitalisation for COVID-19
Abstract
Background: Persistence of respiratory symptoms, particularly breathlessness, after acute coronavirus disease 2019 (COVID-19) infection has emerged as a significant clinical problem. We aimed to characterise and identify risk factors for patients with persistent breathlessness following COVID-19 hospitalisation.
Methods: PHOSP-COVID is a multicentre prospective cohort study of UK adults hospitalised for COVID-19. Clinical data were collected during hospitalisation and at a follow-up visit. Breathlessness was measured by a numeric rating scale of 0-10. We defined post-COVID-19 breathlessness as an increase in score of ≥1 compared to the pre-COVID-19 level. Multivariable logistic regression was used to identify risk factors and to develop a prediction model for post-COVID-19 breathlessness.
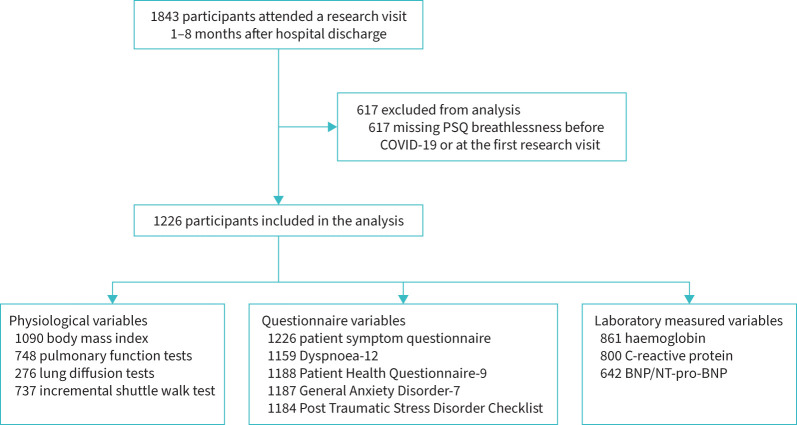
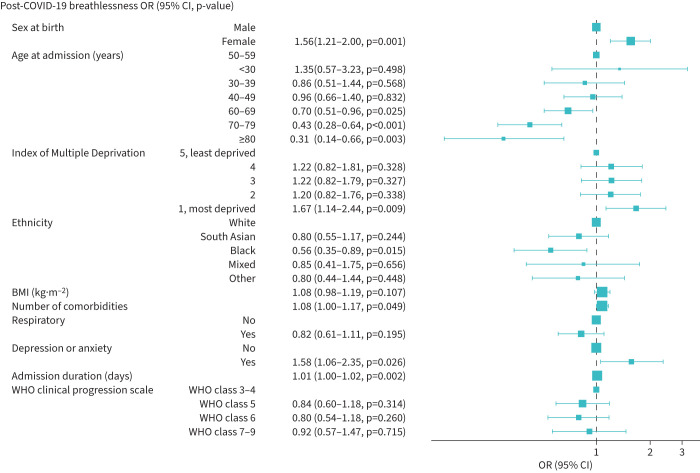
Results: We included 1226 participants (37% female, median age 59 years, 22% mechanically ventilated). At a median 5 months after discharge, 50% reported post-COVID-19 breathlessness. Risk factors for post-COVID-19 breathlessness were socioeconomic deprivation (adjusted OR 1.67, 95% CI 1.14-2.44), pre-existing depression/anxiety (adjusted OR 1.58, 95% CI 1.06-2.35), female sex (adjusted OR 1.56, 95% CI 1.21-2.00) and admission duration (adjusted OR 1.01, 95% CI 1.00-1.02). Black ethnicity (adjusted OR 0.56, 95% CI 0.35-0.89) and older age groups (adjusted OR 0.31, 95% CI 0.14-0.66) were less likely to report post-COVID-19 breathlessness. Post-COVID-19 breathlessness was associated with worse performance on the shuttle walk test and forced vital capacity, but not with obstructive airflow limitation. The prediction model had fair discrimination (concordance statistic 0.66, 95% CI 0.63-0.69) and good calibration (calibration slope 1.00, 95% CI 0.80-1.21).
Conclusions: Post-COVID-19 breathlessness was commonly reported in this national cohort of patients hospitalised for COVID-19 and is likely to be a multifactorial problem with physical and emotional components.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: C.E. Brightling, A. Shikotra and M. Sereno report grants from UKRI–MRC/DHSC–NIHR during the conduct of the study. J.D. Chalmers reports grants and personal fees from AstraZeneca and BI, personal fees from Chiesi, grants from Gilead Sciences, grants and personal fees from GSK and Insmed, personal fees from Janssen, grants and personal fees from Novartis, and personal fees from Zambon outside the submitted work, and is an associate editor of this journal. A. De Soyza reports grants, personal fees and other support from AstraZeneca, Bayer, BI, Chiesi, Forest Labs, GSK, Grifols, Insmed, MedImmune, Novartis, Pfizer and 30T outside the submitted work. R.A. Evans reports grants from UKRI/MRC/NIHR during the conduct of the study and speaker fees from BI. A. Horsley reports funding from NIHR Manchester Biomedical Research Centre, grants from the Cystic Fibrosis Foundation, JP Moulton Trust and NIHR, and personal fees from Vertex Pharmaceuticals and Mylan Healthcare, all outside the submitted work. L.G. Heaney reports support from AstraZeneca, BI, Chiesi, GSK and Napp Pharmaceuticals, personal fees from Novartis, Hoffman la Roche/Genentech Inc., Sanofi, Evelo Biosciences, GSK, AstraZeneca, Teva, Theravance and Circassia, grants from Medimmune, Novartis UK, Roche/Genetech Inc and GSK, Amgen, Genetech/Hoffman la Roche, AZ, Medimmune, GSK, Aerocrine and Vitalograph, outside the submitted work. J.R. Hurst reports grants, personal fees and nonfinancial support from pharmaceutical companies that make medicines to treat respiratory disease, outside the submitted work. G. Jenkins reports grants from GSK, grants and personal fees from Pliant Therapeutics, and grants from Biogen, during the conduct of the study; personal fees from Galapagos, other support from Galecto, personal fees and other support from GSK and AstraZeneca, personal fees from Boehringer Ingelheim, Pliant, Bristol Myers Squibb, Chiesi and Roche/Promedior, personal fees and other support from RedX, other support from NuMedii and Nordic Biosciences, personal fees from Veracyte, PatientMPower, Resolution Therapeutics and Vicore, outside the submitted work; and is supported by a National Institute of Health Research Professorship (NIHR ref. RP-2017-08-ST2-014) and is trustee for Action for Pulmonary Fibrosis. P. Pfeffer reports grants from NIHR outside the submitted work. J.K. Quint reports grants and personal fees from AstraZeneca, grants from Bayer, grants and personal fees from BI, Chiesi and GSK, grants from MRC, The Health Foundation and AUK/BLF, outside the submitted work. B. Raman is supported by the British Heart Foundation Oxford Centre of Research Excellence (RE/18/3/34214). A. Sheikh reports grants from HDRUK, NIHR, MRC and ICSF, during the conduct of the study; and is a Member of the Scottish Government's CMO COVID-19 Advisory Group and Standing Committee on Pandemics. A. Singapuri reports grants from MRC during the conduct of the study. S. Siddiqui reports grants from NIHR Leicester Biomedical Research Centre and NIHR PHOSP COVID, personal fees from AstraZeneca, GSK, CSL Behring, Knopp Biosciences, Owlstone Medical and Chiesi, outside the submitted work; and has a patent pending for volatile breath biomarkers of breathlessness. M. Toshner reports personal fees from Actelion/J&J and GSK, and other support from Morphogen-IX, outside the submitted work. L.V. Wain reports grants from GSK and Orion, outside the submitted work. All other authors declare no competing interests.
Figures
Similar articles
-
Effects of sleep disturbance on dyspnoea and impaired lung function following hospital admission due to COVID-19 in the UK: a prospective multicentre cohort study.Lancet Respir Med. 2023 Aug;11(8):673-684. doi: 10.1016/S2213-2600(23)00124-8. Epub 2023 Apr 15. Lancet Respir Med. 2023. PMID: 37072018 Free PMC article.
-
Persistent symptoms and clinical findings in adults with post-acute sequelae of COVID-19/post-COVID-19 syndrome in the second year after acute infection: A population-based, nested case-control study.PLoS Med. 2025 Jan 23;22(1):e1004511. doi: 10.1371/journal.pmed.1004511. eCollection 2025 Jan. PLoS Med. 2025. PMID: 39847575 Free PMC article.
-
Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study.Lancet Respir Med. 2021 Nov;9(11):1275-1287. doi: 10.1016/S2213-2600(21)00383-0. Epub 2021 Oct 7. Lancet Respir Med. 2021. PMID: 34627560 Free PMC article.
-
Case-finding and improving patient outcomes for chronic obstructive pulmonary disease in primary care: the BLISS research programme including cluster RCT.Southampton (UK): NIHR Journals Library; 2021 Nov. Southampton (UK): NIHR Journals Library; 2021 Nov. PMID: 34780128 Free Books & Documents. Review.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Prognostic Factors for Predicting Post-COVID-19 Condition in Patients With COVID-19 in an Outpatient Setting.J Korean Med Sci. 2024 Jan 15;39(2):e23. doi: 10.3346/jkms.2024.39.e23. J Korean Med Sci. 2024. PMID: 38225786 Free PMC article.
-
Exploring the Experience of Breathlessness with the Common-Sense Model of Self-Regulation (CSM).Healthcare (Basel). 2023 Jun 8;11(12):1686. doi: 10.3390/healthcare11121686. Healthcare (Basel). 2023. PMID: 37372804 Free PMC article.
-
Proteomic Evolution from Acute to Post-COVID-19 Conditions.J Proteome Res. 2024 Jan 5;23(1):52-70. doi: 10.1021/acs.jproteome.3c00324. Epub 2023 Dec 4. J Proteome Res. 2024. PMID: 38048423 Free PMC article.
-
Effect of immunoadsorption on clinical presentation and immune alterations in COVID-19-induced and/or aggravated ME/CFS.Mol Ther. 2025 Jun 4;33(6):2886-2899. doi: 10.1016/j.ymthe.2025.01.007. Epub 2025 Jan 10. Mol Ther. 2025. PMID: 39797400
-
Predictors of reduced incremental shuttle walk test performance in patients with long post-COVID-19.J Bras Pneumol. 2024 Jan 15;49(6):e20220438. doi: 10.36416/1806-3756/e20220438. eCollection 2024. J Bras Pneumol. 2024. PMID: 38232250 Free PMC article.
References
-
- World Health Organization . COVID-19 Weekly Epidemiological Update. https://www.who.int/publications/m/item/weekly-epidemiological-update-on.... Date last updated: 1 June 2022. Date last accessed: 1 June 2022.
-
- National Institute for Health and Care Excellence . COVID-19 rapid guideline: managing the long-term effects of COVID-19. NICE guideline [NG188]. https://www.nice.org.uk/guidance/ng188. Date last updated: 11 November 2021. Date last accessed: 7 June 2022. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources