

Outcomes after the Ross procedure with pulmonary autograft reinforcement by reimplantation
- PMID: 36820346
- PMCID: PMC9938391
- DOI: 10.1016/j.xjtc.2022.11.016
Outcomes after the Ross procedure with pulmonary autograft reinforcement by reimplantation
Abstract
Background: Pulmonary autograft reinforcement to prevent dilatation and subsequent neo-aortic valve regurgitation has been reported; however, data on long-term function of the neo-aortic valve after this modified Ross procedure are lacking. Our objective here was to assess long-term outcomes of the modified Ross procedure with autograft reinforcement using the reimplantation technique.
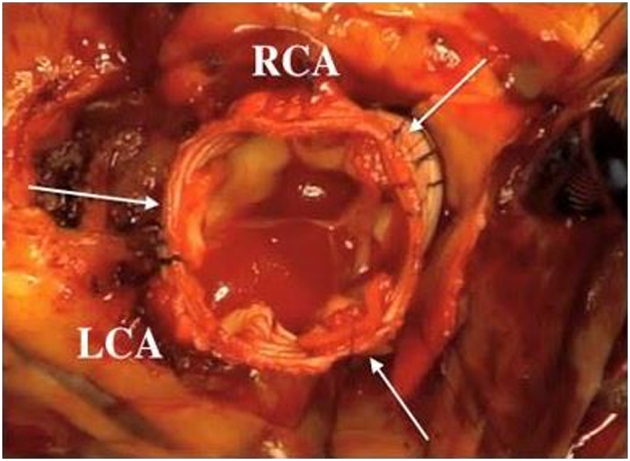
Patients: The outcomes of 61 consecutive patients managed using the Dacron-conduit reinforced Ross procedure between 2009 and 2021 were reviewed. Most patients had a unicuspid or bicuspid aortic valve (n = 52; 85%), predominant aortic valve regurgitation (n = 42; 77%), and >30 mm dilatation of the ascending aorta (n = 33; 54%). A prior aortic valve procedure was noted in 47 patients (77%) patients, including 38 (62%) with surgical repair and 9 (15%) with balloon dilatation. The pulmonary autograft was reimplanted within a Dacron conduit with a median diameter of 25.6 mm (range, 20-30 mm) using the David valve-sparing aortic root replacement technique.
Results: All patients survived. The median age at surgery was 16.8 years (range, 6-38 years). Neo-aortic valve replacement was required in 3 patients (4.9%; 95% CI, 0.34%- 12.7%) because of infective endocarditis, left ventricular false aneurysm, and leaflet perforation, respectively; the repeat procedure was done early in 2 of these patients (2 of 61; 3%). Six patients required right ventricular outflow conduit replacement, 5 by surgery and 1 percutaneously. The median duration of follow-up was 90 months (range, 10-124 months). The 5- and 10-year rates of reintervention-free survival were 84.3% (95% CI, 74%-95%) and 81.6% (95% CI, 72%-93%), respectively, and 5-year survival without aortic reintervention was 94.5% (95% CI, 88%-100%), with little change at 10 years. No patients experienced deterioration of initial neo-aortic valve function (ie, regurgitation or stenosis).
Conclusions: Autograft reinforcement using the reimplantation technique allowed expansion of Ross procedure indications to all patients requiring aortic valve replacement and prevented neo-aortic root dilatation. Failures were uncommon. Long-term follow-up data showed stable neo-aortic valve function.
Keywords: CT, computed tomography; Ross procedure; aortic valve repair; congenital heart disease.
© 2023 The Authors.
Figures







Similar articles
-
The Ross procedure in children and young adults with congenital aortic valve disease.J Heart Valve Dis. 1997 Jul;6(4):335-42. J Heart Valve Dis. 1997. PMID: 9263860
-
The Ross procedure: long-term clinical and echocardiographic follow-up.Ann Thorac Surg. 2004 Sep;78(3):773-81; discussion 773-81. doi: 10.1016/j.athoracsur.2004.02.033. Ann Thorac Surg. 2004. PMID: 15336990
-
Long-Term Clinical and Imaging Follow-Up After Reinforced Pulmonary Autograft Ross Procedure.Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2016;19(1):59-62. doi: 10.1053/j.pcsu.2015.11.005. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2016. PMID: 27060045 Review.
-
Reoperations after the ross procedure in adults: towards autograft-sparing/Ross reversal.J Heart Valve Dis. 2011 Jul;20(4):425-32. J Heart Valve Dis. 2011. PMID: 21863656
-
[Indications for and clinical outcome of the Ross procedure: a review].Nihon Geka Gakkai Zasshi. 2001 Apr;102(4):330-6. Nihon Geka Gakkai Zasshi. 2001. PMID: 11344686 Review. Japanese.
References
-
- Bouhout I., Ghoneim A., Tousch M., Stevens L.M., Semplonius T., Tarabzoni M., et al. Impact of a tailored surgical approach on autograft root dimensions in patients undergoing the Ross procedure for aortic regurgitation. Eur J Cardiothorac Surg. 2019;56:959–967. doi: 10.1093/ejcts/ezz105. - DOI - PubMed
LinkOut - more resources
Full Text Sources
