

A shallow morphology of the intertubercular groove is associated with medial and bilateral but not lateral pulley lesions
- PMID: 36820903
- PMCID: PMC10356675
- DOI: 10.1007/s00167-023-07350-x
A shallow morphology of the intertubercular groove is associated with medial and bilateral but not lateral pulley lesions
Abstract
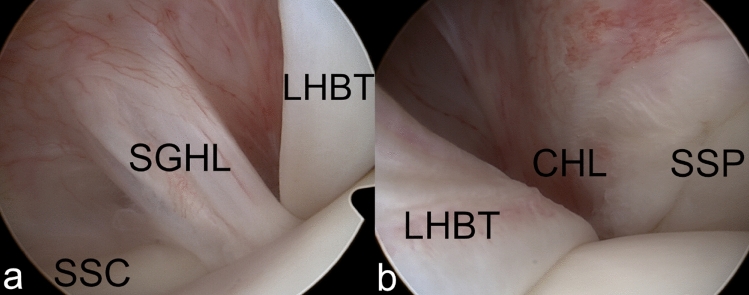
Purpose: To investigate the influence of intertubercular groove (IG) morphology on the development of different types of biceps reflection pulley (BRP) injuries.
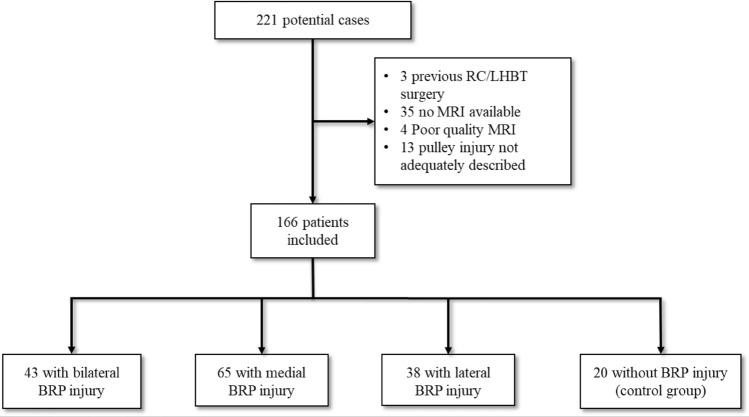
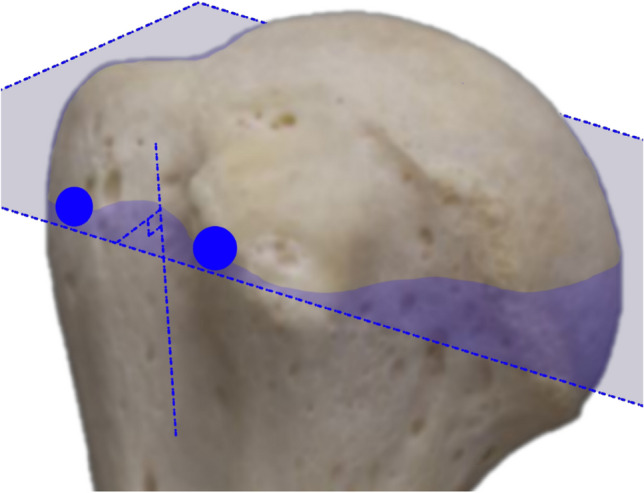
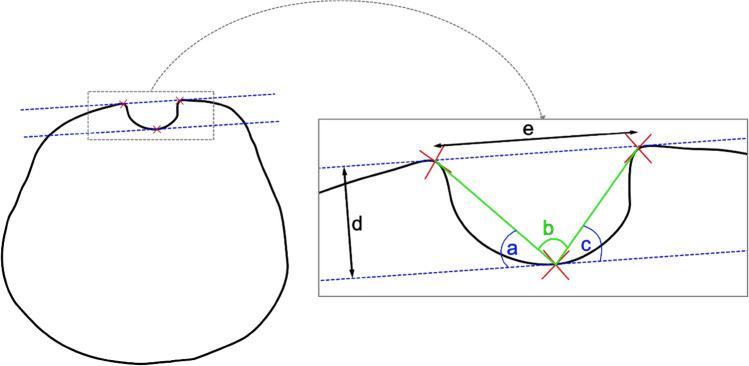
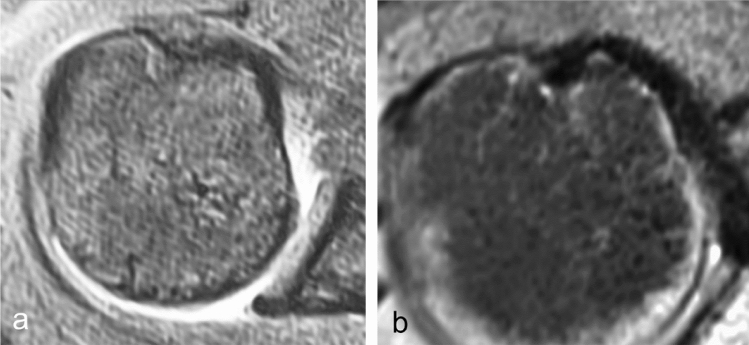
Methods: A consecutive cohort of 221 patients with ventral shoulder pain and a preoperative diagnosis suspecting BRP injury, who underwent arthroscopy, was retrospectively reviewed. The presence or absence as well as type of pulley injury (medial, lateral or bilateral) was confirmed arthroscopically. The intertubercular groove was evaluated on MRIs after triplanar reconstruction of the axial plane. IG depth, width, medial wall angle (MWA), lateral wall angle (LWA) and total opening angle (TOA) were measured. IG depth and width were expressed in relation to the humeral head diameter. Measurements were performed by two clinicians independently and averaged.
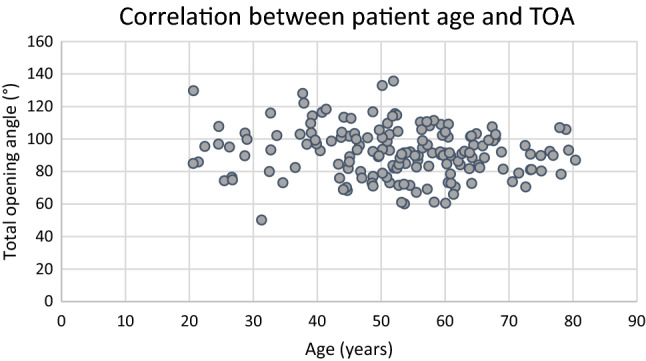
Results: Of 166 included patients 43 had bilateral, 65 medial and 38 lateral BRP lesions. 20 patients had intact BRPs and represented the control group. The intra-class correlation coefficient of measurements was 0.843-0.955. Patients with a medial or bilateral BRP injury had a flatter MWA (38.8° or 40.0° vs. 47.9°, p < 0.001), wider TOA (96.1° or 96.6° vs. 82.6°, p < 0.001), greater width (12.5 or 12.3 vs. 10.8 mm, p = 0.013) and shallower depth (5.5 or 5.4 vs. 6.2 mm, p < 0.001) than the control group. Conversely, the IG morphology of those with lateral BRP injuries did not differ significantly from the control group. The odds ratio for a medial or bilateral BRP injury when the TOA exceeded 95° was 6.8 (95% confidence interval 3.04-15.2).
Conclusion: A dysplastic type of IG morphology with a wide TOA, flat MWA, decreased depth and increased width is associated with the presence of medial and bilateral BRP injuries. A TOA of > 95° increases the likelihood of a medial or bilateral BRP injury 6.8-fold. Lateral BRP injuries are not associated with dysplastic IG morphology. Concomitant LHBT surgery may, therefore, not always be necessary during isolated supraspinatus tendon repair.
Level of evidence: Level III.
Keywords: Biceps reflection pulley; Dysplastic; Influencing factor; Intertubercular groove morphology; Rotator cuff.
© 2023. The Author(s).
Conflict of interest statement
No conflict of interest pertaining to the subject of this manuscript is declared by any of the authors.
Figures
Similar articles
-
Correlation between the morphological features of the biceps groove and injuries to the biceps pulley and the long head tendon of the biceps.BMC Musculoskelet Disord. 2023 May 12;24(1):377. doi: 10.1186/s12891-023-06497-5. BMC Musculoskelet Disord. 2023. PMID: 37173699 Free PMC article.
-
Morphology of the Lesser Tuberosity and Intertubercular Groove in Patients With Arthroscopically Confirmed Subscapularis and Biceps Tendon Pathology.Arthroscopy. 2016 Jun;32(6):968-75. doi: 10.1016/j.arthro.2015.11.035. Epub 2016 Feb 11. Arthroscopy. 2016. PMID: 26874801
-
The effect of bicipital groove morphology on the stability of the biceps long head tendon.Arch Orthop Trauma Surg. 2021 Aug;141(8):1325-1330. doi: 10.1007/s00402-021-03760-z. Epub 2021 Jan 23. Arch Orthop Trauma Surg. 2021. PMID: 33484303
-
Proximal Biceps Tendon and Rotator Cuff Tears.Clin Sports Med. 2016 Jan;35(1):153-61. doi: 10.1016/j.csm.2015.08.010. Epub 2015 Sep 26. Clin Sports Med. 2016. PMID: 26614474 Review.
-
Multimedia article. The rotator interval: pathology and management.Arthroscopy. 2011 Apr;27(4):556-67. doi: 10.1016/j.arthro.2010.10.004. Epub 2011 Feb 4. Arthroscopy. 2011. PMID: 21295939 Review.
Cited by
-
Is the Tendon-to-Groove Ratio Associated with Elevated Risk for LHB Tendon Disorders?-A New Approach of Preoperative MR-Graphic Analysis for Targeted Diagnosis of Tendinopathy of the Long Head of Biceps.J Clin Med. 2024 May 13;13(10):2860. doi: 10.3390/jcm13102860. J Clin Med. 2024. PMID: 38792401 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
