

Cryptococcal Meningitis and Clinical Outcomes in Persons With Human Immunodeficiency Virus: A Global View
- PMID: 36821489
- PMCID: PMC10273391
- DOI: 10.1093/cid/ciad076
Cryptococcal Meningitis and Clinical Outcomes in Persons With Human Immunodeficiency Virus: A Global View
Abstract
Background: Cryptococcal meningitis (CM) is a major cause of morbidity and mortality in persons with human immunodeficiency virus (HIV; PWH). Little is known about CM outcomes and availability of diagnostic and treatment modalities globally.
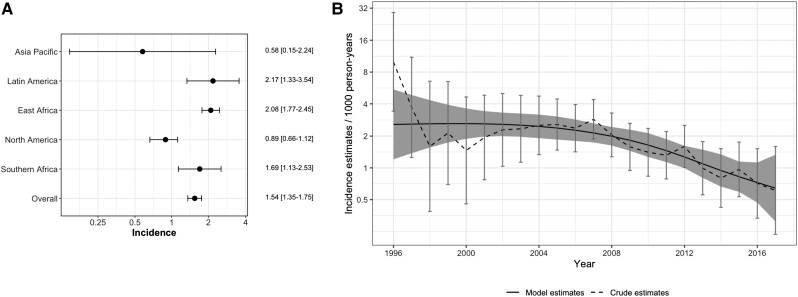
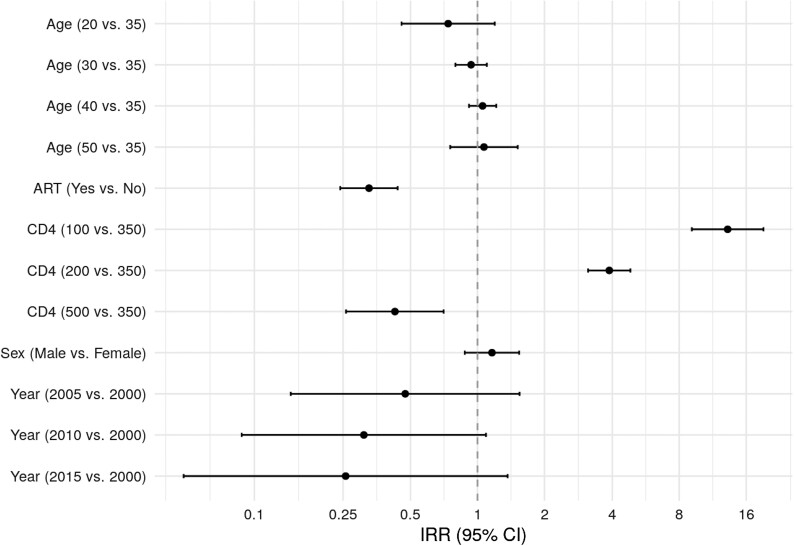
Methods: In this retrospective cohort study, we investigated CM incidence and all-cause mortality in PWH in the International Epidemiology Databases to Evaluate AIDS cohort from 1996 to 2017. We estimated incidence using quasi-Poisson models adjusted for sex, age, calendar year, CD4 cell count (CD4), and antiretroviral therapy (ART) status. Mortality after CM diagnosis was examined using multivariable Cox models. A site survey from 2017 assessed availability of CM diagnostic and treatment modalities.
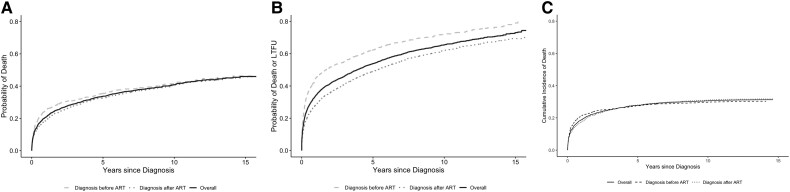
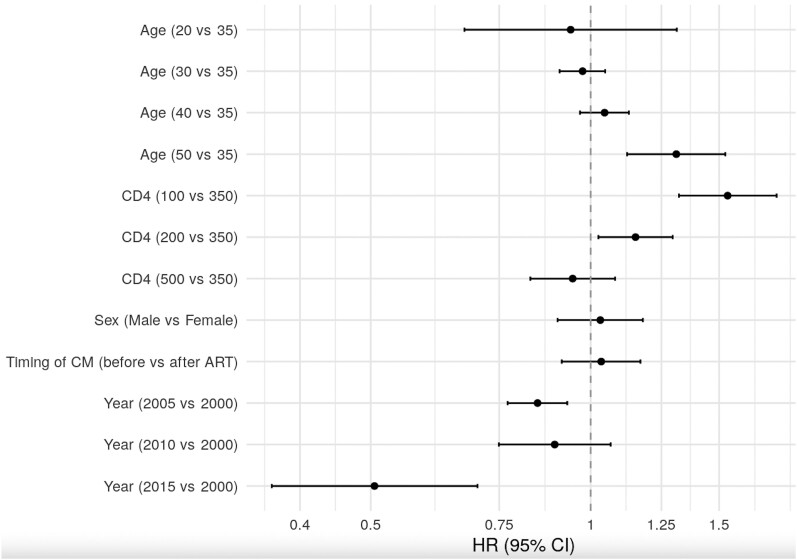
Results: Among 518 852 PWH, there were 3857 cases of CM with an estimated incidence of 1.54 per 1000 person-years. Mortality over a median of 2.6 years of post-CM diagnosis follow-up was 31.6%, with 29% lost to follow-up. In total, 2478 (64%) were diagnosed with CM after ART start with a median of 253 days from ART start to CM diagnosis. Older age (hazard [HR], 1.31 for 50 vs 35 years), lower CD4 (HR, 1.15 for 200 vs 350 cells/mm3), and earlier year of CM diagnosis (HR, 0.51 for 2015 vs 2000) were associated with higher mortality. Of 89 sites, 34% reported access to amphotericin B; 12% had access to flucytosine.
Conclusions: Mortality after CM diagnosis was high. A substantial portion of CM cases occurred after ART start, though incidence and mortality may be higher than reported due to ascertainment bias. Many sites lacked access to recommended CM treatment.
Keywords: AIDS; HIV; cryptococcal meningitis; global health.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. M. J. G. reports an NIH subgrant from JSPHU to the University of Calgary and honoraria for participation as an ad hoc member of HIV Canadian advisory boards to Merck, ViiV Healthcare, and Gilead. G. W. reports unrestricted research grants from Roche Diagnostics and Gilead Sciences and honoraria for advisory board participation and/or travel grants from MSD, Gilead Sciences, and ViiV Healthcare, all paid to their institution. A. K. P. reports participation on the HIV Medicine Association Board of Directors and receipt of support for attending meetings and/or travel including Vanderbilt continuing medical education funds. C. C. M. reports support for attending meetings and/or travel from NIH paid to their institution. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Molloy SF, Kanyama C, Heyderman RS, et al. Antifungal combinations for treatment of cryptococcal meningitis in Africa. N Engl J Med 2018; 378:1004–17. - PubMed
-
- Lawrence DS, Boyer-Chammard T, Jarvis JN. Emerging concepts in HIV-associated cryptococcal meningitis. Curr Opin Infect Dis 2019; 32:16–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
