

Novel Note Templates to Enhance Signal and Reduce Noise in Medical Documentation: Prospective Improvement Study
- PMID: 36821760
- PMCID: PMC10134024
- DOI: 10.2196/41223
Novel Note Templates to Enhance Signal and Reduce Noise in Medical Documentation: Prospective Improvement Study
Abstract
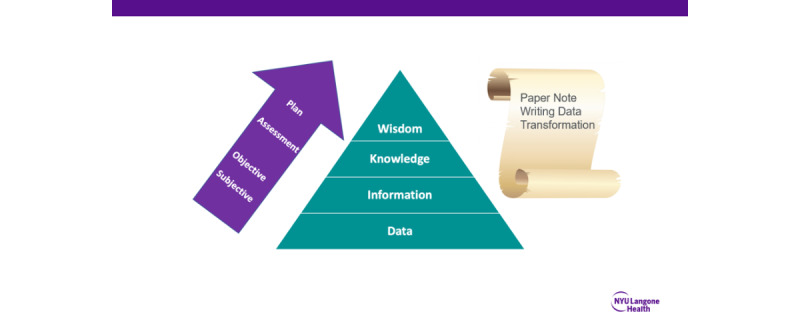
Background: The introduction of electronic workflows has allowed for the flow of raw uncontextualized clinical data into medical documentation. As a result, many electronic notes have become replete of "noise" and deplete clinically significant "signals." There is an urgent need to develop and implement innovative approaches in electronic clinical documentation that improve note quality and reduce unnecessary bloating.
Objective: This study aims to describe the development and impact of a novel set of templates designed to change the flow of information in medical documentation.
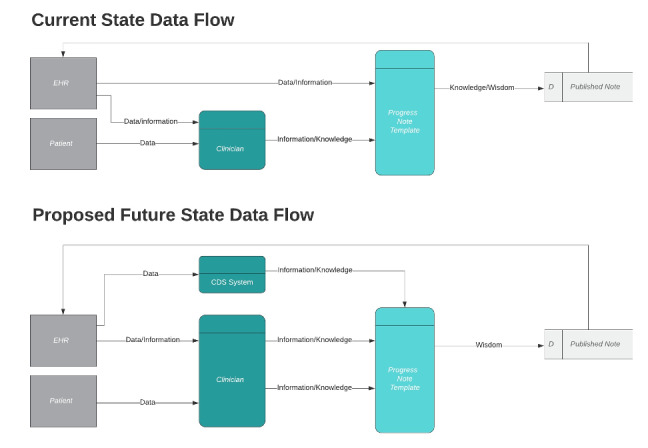
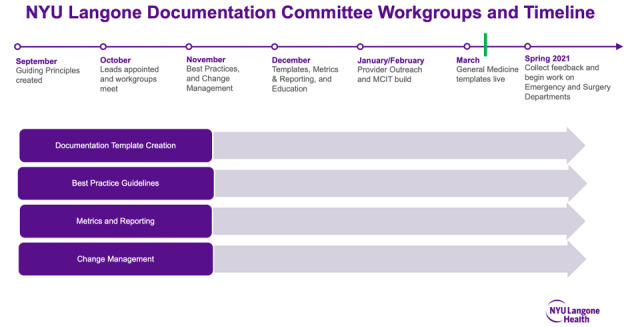
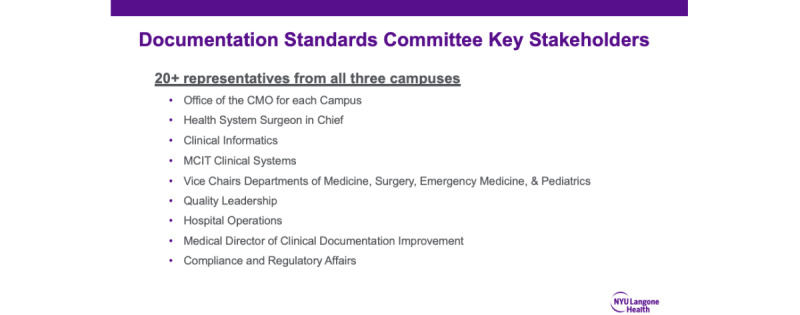
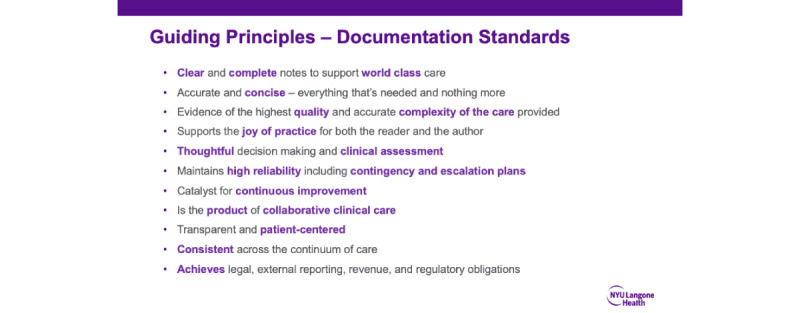
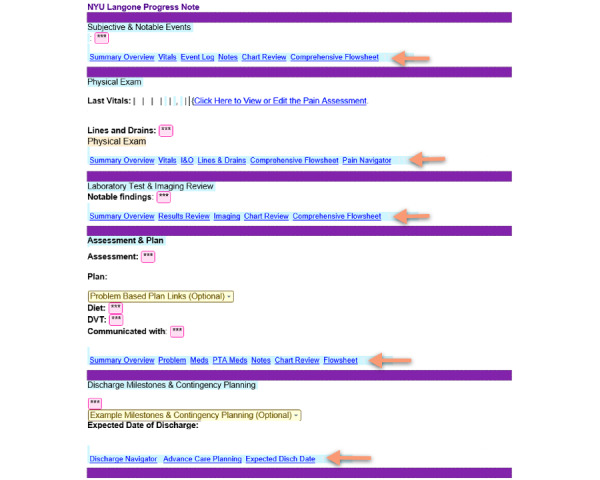
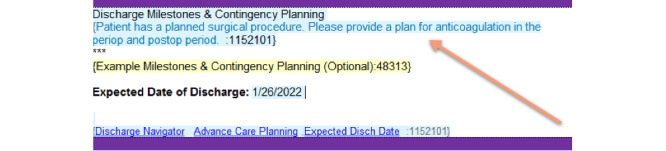
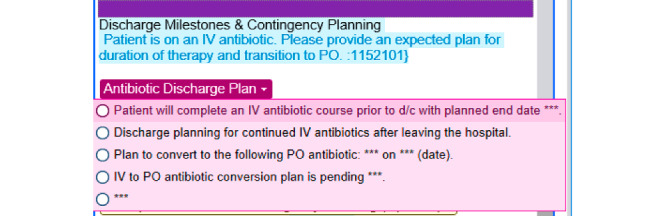
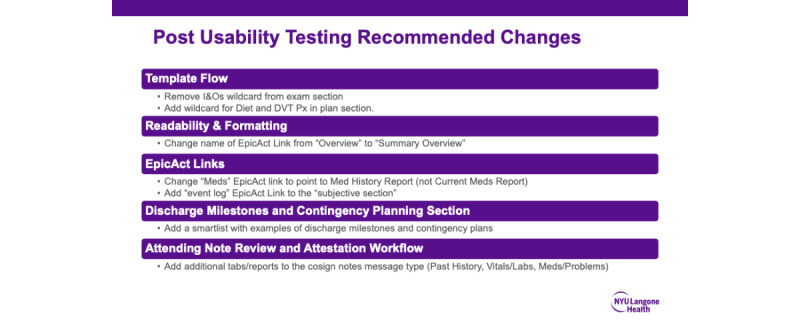
Methods: This is a multihospital nonrandomized prospective improvement study conducted on the inpatient general internal medicine service across 3 hospital campuses at the New York University Langone Health System. A group of physician leaders representing each campus met biweekly for 6 months. The output of these meetings included (1) a conceptualization of the note bloat problem as a dysfunction in information flow, (2) a set of guiding principles for organizational documentation improvement, (3) the design and build of novel electronic templates that reduced the flow of extraneous information into provider notes by providing link outs to best practice data visualizations, and (4) a documentation improvement curriculum for inpatient medicine providers. Prior to go-live, pragmatic usability testing was performed with the new progress note template, and the overall user experience was measured using the System Usability Scale (SUS). Primary outcome measures after go-live include template utilization rate and note length in characters.
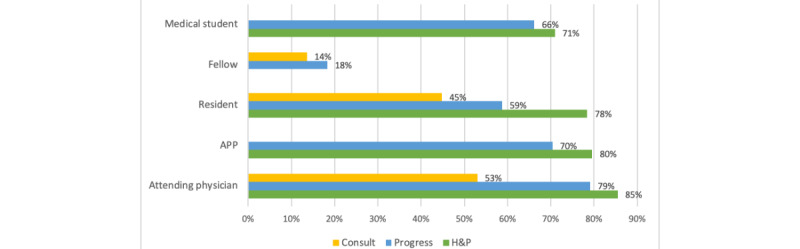
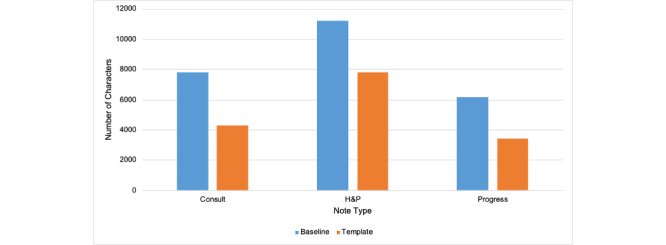
Results: In usability testing among 22 medicine providers, the new progress note template averaged a usability score of 90.6 out of 100 on the SUS. A total of 77% (17/22) of providers strongly agreed that the new template was easy to use, and 64% (14/22) strongly agreed that they would like to use the template frequently. In the 3 months after template implementation, general internal medicine providers wrote 67% (51,431/76,647) of all inpatient notes with the new templates. During this period, the organization saw a 46% (2768/6191), 47% (3505/7819), and 32% (3427/11,226) reduction in note length for general medicine progress notes, consults, and history and physical notes, respectively, when compared to a baseline measurement period prior to interventions.
Conclusions: A bundled intervention that included the deployment of novel templates for inpatient general medicine providers significantly reduced average note length on the clinical service. Templates designed to reduce the flow of extraneous information into provider notes performed well during usability testing, and these templates were rapidly adopted across all hospital campuses. Further research is needed to assess the impact of novel templates on note quality, provider efficiency, and patient outcomes.
Keywords: clinical documentation; clinical informatics; decision support; hospital data; medical informatics.
©Jonah Feldman, Adam Goodman, Katherine Hochman, Eesha Chakravartty, Jonathan Austrian, Eduardo Iturrate, Brian Bosworth, Archana Saxena, Marwa Moussa, Dina Chenouda, Frank Volpicelli, Nicole Adler, Joseph Weisstuch, Paul Testa. Originally published in JMIR Formative Research (https://formative.jmir.org), 12.04.2023.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Rule A, Bedrick S, Chiang MF, Hribar MR. Length and redundancy of outpatient progress notes across a decade at an academic medical center. JAMA Netw Open. 2021 Jul 01;4(7):e2115334. doi: 10.1001/jamanetworkopen.2021.15334. https://europepmc.org/abstract/MED/34279650 2782054 - DOI - PMC - PubMed
-
- Kuhn T, Basch P, Barr M, Yackel T, Medical Informatics Committee of the American College of Physicians Clinical documentation in the 21st century: executive summary of a policy position paper from the American College of Physicians. Ann Intern Med. 2015;162(4):301–303. doi: 10.7326/M14-2128. https://www.acpjournals.org/doi/abs/10.7326/M14-2128?url_ver=Z39.88-2003... 2089368 - DOI - DOI - PubMed
-
- Goldstein IH, Hwang T, Gowrisankaran S, Bales R, Chiang MF, Hribar MR. Changes in electronic health record use time and documentation over the course of a decade. Ophthalmology. 2019;126(6):783–791. doi: 10.1016/j.ophtha.2019.01.011. https://europepmc.org/abstract/MED/30664893 S0161-6420(18)32509-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
