

Optimal Intensity and Duration of Walking Rehabilitation in Patients With Chronic Stroke: A Randomized Clinical Trial
- PMID: 36822187
- PMCID: PMC9951105
- DOI: 10.1001/jamaneurol.2023.0033
Optimal Intensity and Duration of Walking Rehabilitation in Patients With Chronic Stroke: A Randomized Clinical Trial
Abstract
Importance: For walking rehabilitation after stroke, training intensity and duration are critical dosing parameters that lack optimization.
Objective: To assess the optimal training intensity (vigorous vs moderate) and minimum training duration (4, 8, or 12 weeks) needed to maximize immediate improvement in walking capacity in patients with chronic stroke.
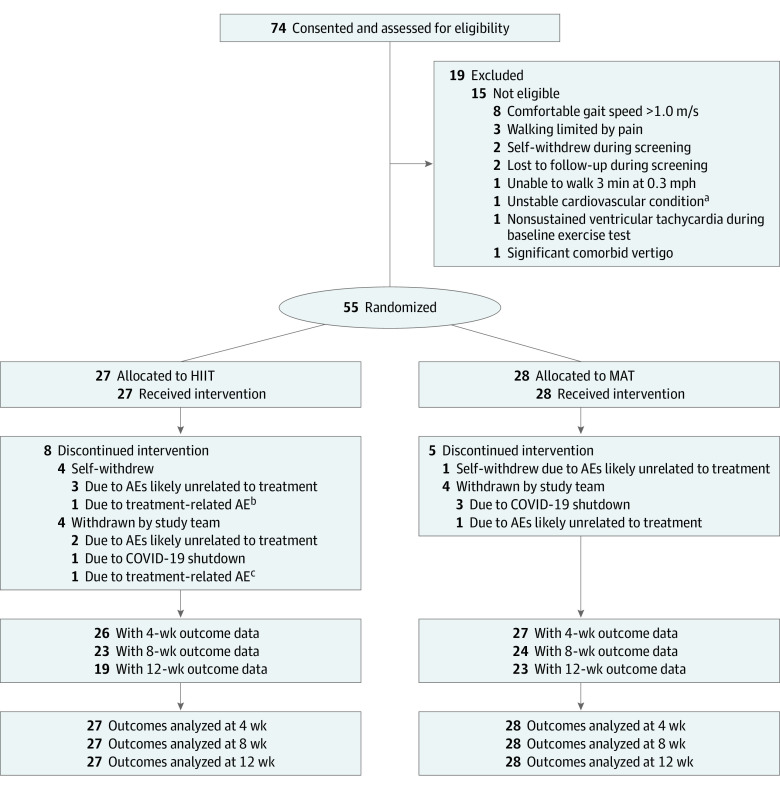
Design, setting, and participants: This multicenter randomized clinical trial using an intent-to-treat analysis was conducted from January 2019 to April 2022 at rehabilitation and exercise research laboratories. Survivors of a single stroke who were aged 40 to 80 years and had persistent walking limitations 6 months or more after the stroke were enrolled.
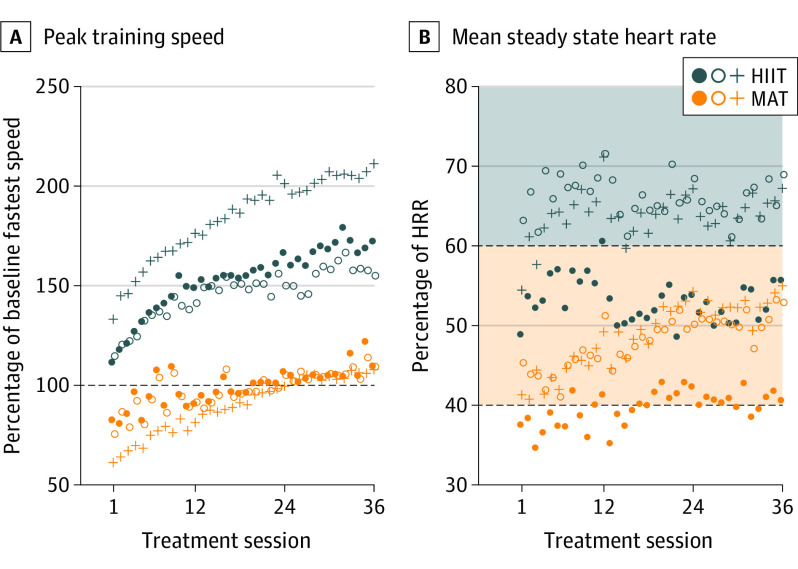
Interventions: Participants were randomized 1:1 to high-intensity interval training (HIIT) or moderate-intensity aerobic training (MAT), each involving 45 minutes of walking practice 3 times per week for 12 weeks. The HIIT protocol used repeated 30-second bursts of walking at maximum safe speed, alternated with 30- to 60-second rest periods, targeting a mean aerobic intensity above 60% of the heart rate reserve (HRR). The MAT protocol used continuous walking with speed adjusted to maintain an initial target of 40% of the HRR, progressing up to 60% of the HRR as tolerated.
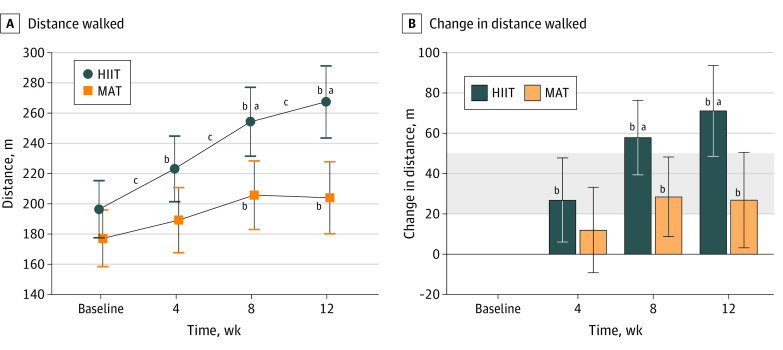
Main outcomes and measures: The main outcome was 6-minute walk test distance. Outcomes were assessed by blinded raters after 4, 8, and 12 weeks of training.
Results: Of 55 participants (mean [SD] age, 63 [10] years; 36 male [65.5%]), 27 were randomized to HIIT and 28 to MAT. The mean (SD) time since stroke was 2.5 (1.3) years, and mean (SD) 6-minute walk test distance at baseline was 239 (132) m. Participants attended 1675 of 1980 planned treatment visits (84.6%) and 197 of 220 planned testing visits (89.5%). No serious adverse events related to study procedures occurred. Groups had similar 6-minute walk test distance changes after 4 weeks (HIIT, 27 m [95% CI, 6-48 m]; MAT, 12 m [95% CI, -9 to 33 m]; mean difference, 15 m [95% CI, -13 to 42 m]; P = .28), but HIIT elicited greater gains after 8 weeks (58 m [95% CI, 39-76 m] vs 29 m [95% CI, 9-48 m]; mean difference, 29 m [95% CI, 5-54 m]; P = .02) and 12 weeks (71 m [95% CI, 49-94 m] vs 27 m [95% CI, 3-50 m]; mean difference, 44 m [95% CI, 14-74 m]; P = .005) of training; HIIT also showed greater improvements than MAT on some secondary measures of gait speed and fatigue.
Conclusions and relevance: These findings show proof of concept that vigorous training intensity is a critical dosing parameter for walking rehabilitation. In patients with chronic stroke, vigorous walking exercise produced significant and meaningful gains in walking capacity with only 4 weeks of training, but at least 12 weeks were needed to maximize immediate gains.
Trial registration: ClinicalTrials.gov Identifier: NCT03760016.
Conflict of interest statement
Figures
Comment in
-
Stepping Closer to Precision Rehabilitation.JAMA Neurol. 2023 Apr 1;80(4):339-341. doi: 10.1001/jamaneurol.2023.0044. JAMA Neurol. 2023. PMID: 36822188 No abstract available.
References
-
- Billinger SA, Arena R, Bernhardt J, et al. ; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Lifestyle and Cardiometabolic Health; Council on Epidemiology and Prevention; Council on Clinical Cardiology . Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532-2553. doi:10.1161/STR.0000000000000022 - DOI - PubMed
-
- Winstein CJ, Stein J, Arena R, et al. ; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Quality of Care and Outcomes Research . Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169. doi:10.1161/STR.0000000000000098 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
