

CD11b mediates hypertensive cardiac remodeling by regulating macrophage infiltration and polarization
- PMID: 36822392
- PMCID: PMC10770112
- DOI: 10.1016/j.jare.2023.02.010
CD11b mediates hypertensive cardiac remodeling by regulating macrophage infiltration and polarization
Abstract
Introduction: Leukocyte infiltration is an early event during cardiac remodeling frequently leading to heart failure (HF). Integrins mediate leukocyte infiltration during inflammation. However, the importance of specific integrins in hypertensive cardiac remodeling is still unclear.
Objectives: To elucidate the significance of CD11b in hypertensive cardiac remodeling.
Methods: Angiotensin (Ang II) or deoxycorticosterone acetate (DOCA)-salt was used to induce cardiac remodeling in mice of gene knockout (KO), bone marrow (BM) chimera, and the CD11b neutralizing antibody or agonist leukadherin-1 (LA1) treatment.
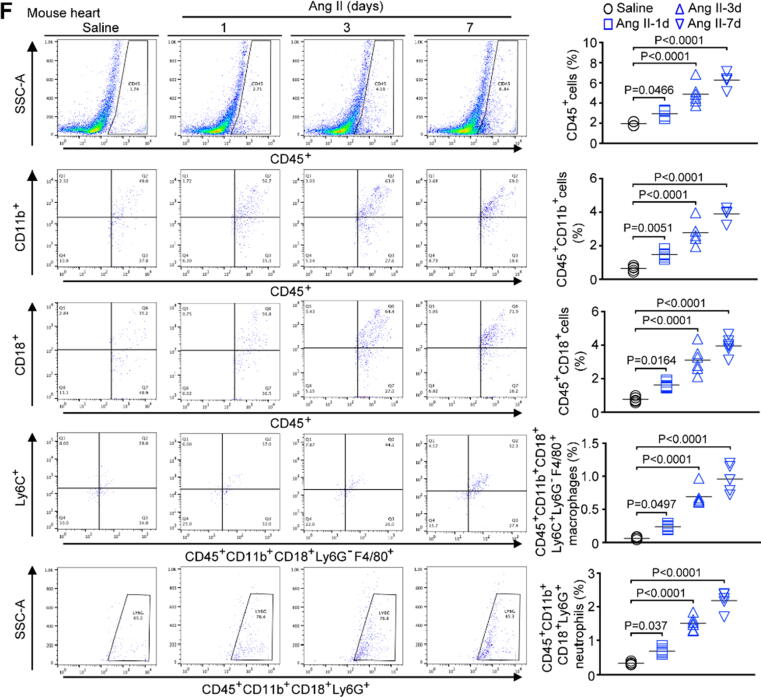
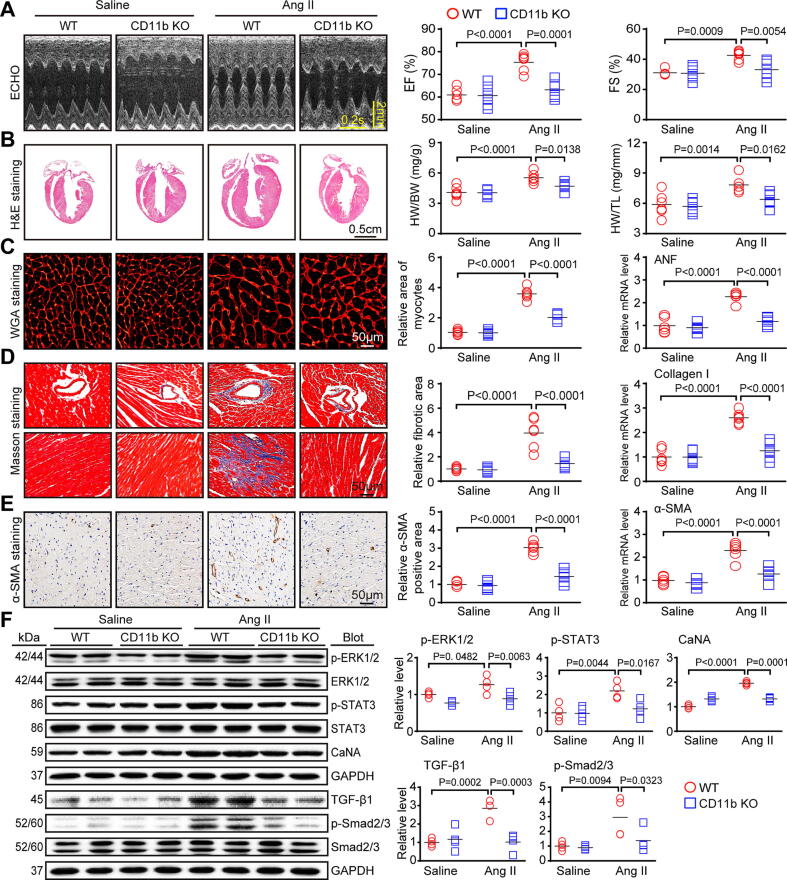
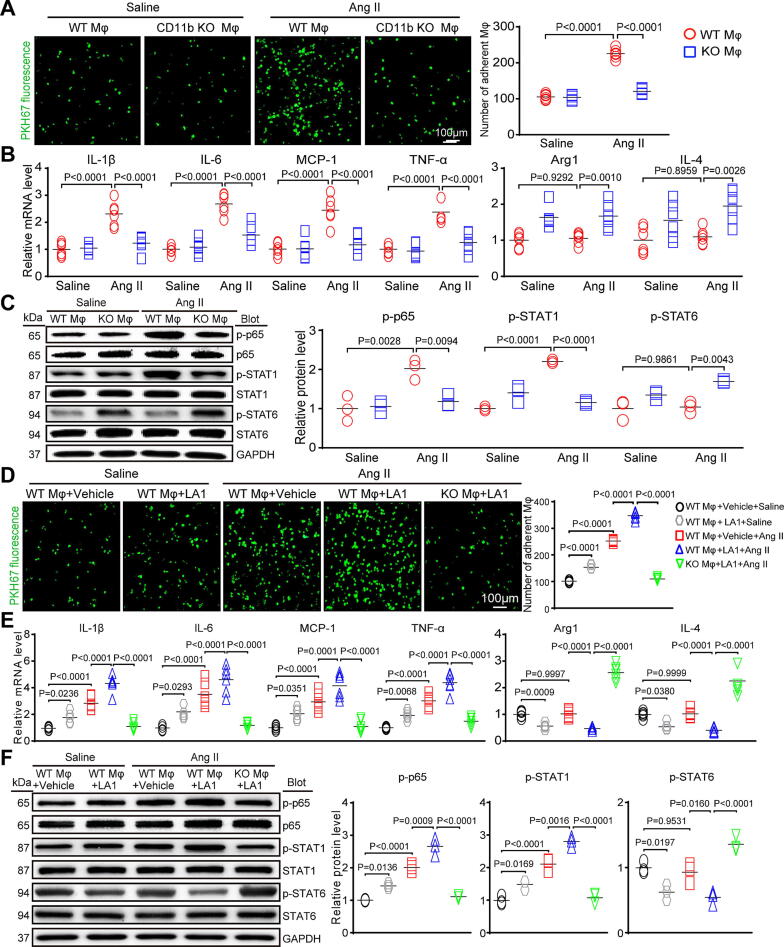
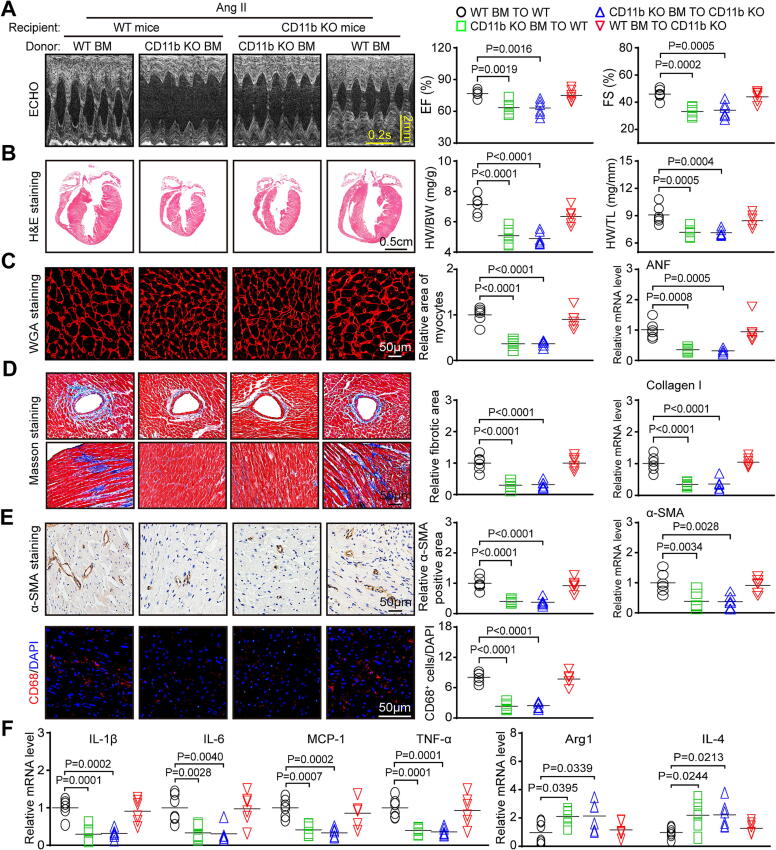
Results: Our microarray data showed that integrin subunits Itgam (CD11b) and Itgb2 (CD18) were the most highly upregulated in Ang II-infused hearts. CD11b expression and CD11b/CD18+ myelomonocytes were also time-dependently increased. KO or pharmacological blockade of CD11b greatly attenuated cardiac remodeling and macrophage infiltration and M1 polarization induced by Ang II or DOCA-salt. This protection was verified in wild-type mice transplanted with CD11b-deficient BM cells. Conversely, administration of CD11b agonist LA1 showed the opposite effects. Further, CD11b KO reduced Ang II-induced macrophage adhesion and M1 polarization, leading to reduction of cardiomyocyte enlargement and fibroblast differentiation in vitro. The numbers of CD14+CD11b+CD18+ monocytes and CD15+CD11b+CD18+ granulocytes were obviously higher in HF patients than in normal controls.
Conclusion: Our data demonstrate an important role of CD11b+ myeloid cells in hypertensive cardiac remodeling, and suggest that HF may benefit from targeting CD11b.
Keywords: Cardiac remodeling; Hypertensive stimuli; Integrin CD11b; Macrophage infiltration and polarization.
Copyright © 2023. Production and hosting by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures






References
-
- González A., Ravassa S., López B., Moreno M.U., Beaumont J., San José G. Myocardial Remodeling in Hypertension. Hypertension. 2018;72(3):549–558. - PubMed
-
- Nwabuo C.C., Vasan R.S. Pathophysiology of Hypertensive Heart Disease: Beyond Left Ventricular Hypertrophy. Curr Hypertens Rep. 2020;22(2):11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
