

Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks
- PMID: 36822570
- PMCID: PMC10363193
- DOI: 10.1016/j.ajo.2023.02.013
Visual Outcomes Following Plasma Exchange for Optic Neuritis: An International Multicenter Retrospective Analysis of 395 Optic Neuritis Attacks
Abstract
Purpose: To evaluate the effectiveness of plasma exchange (PLEX) for optic neuritis (ON).
Methods: We conducted an international multicenter retrospective study evaluating the outcomes of ON following PLEX. Outcomes were compared to raw data from the Optic Neuritis Treatment Trial (ONTT) using a matched subset.
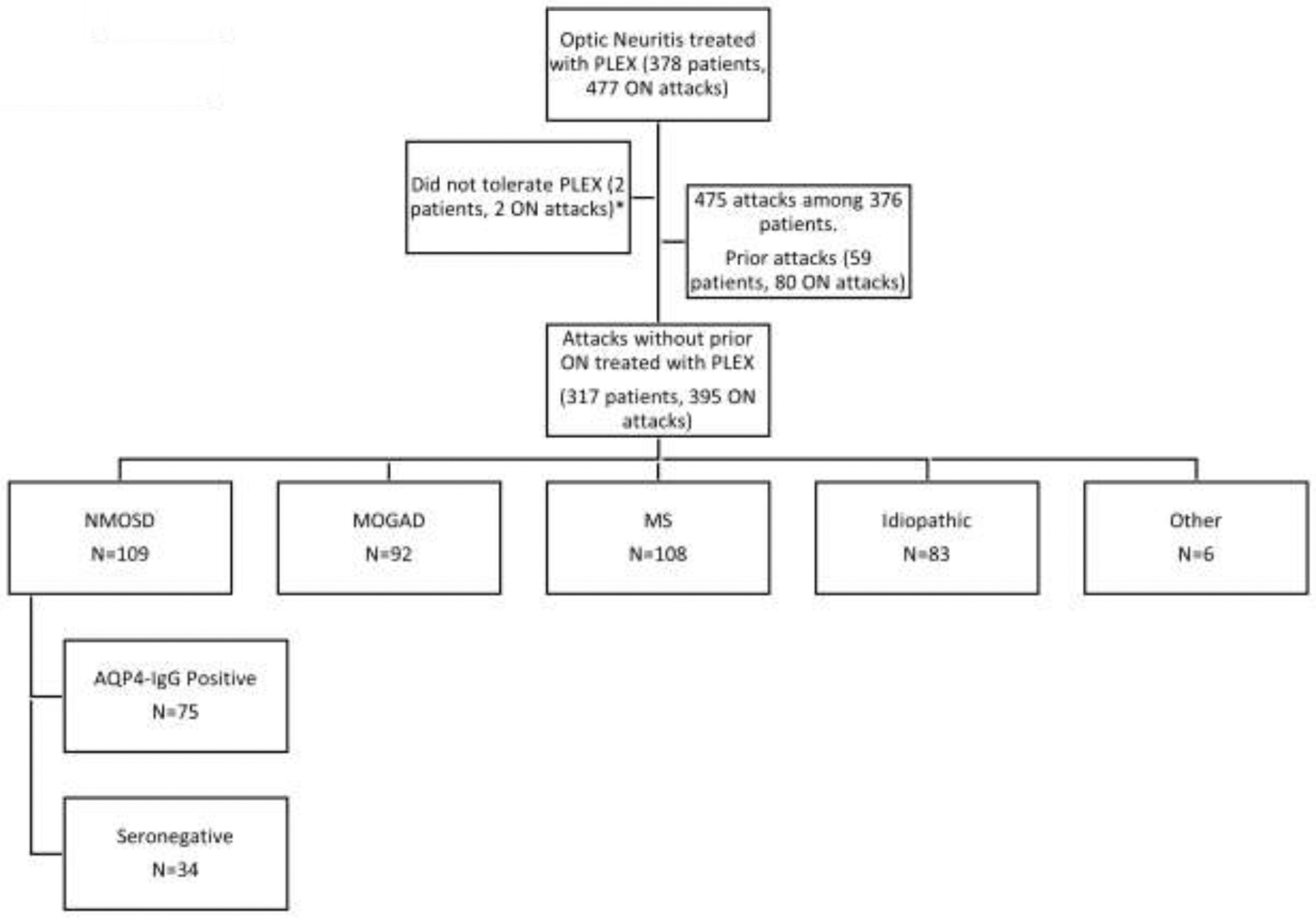
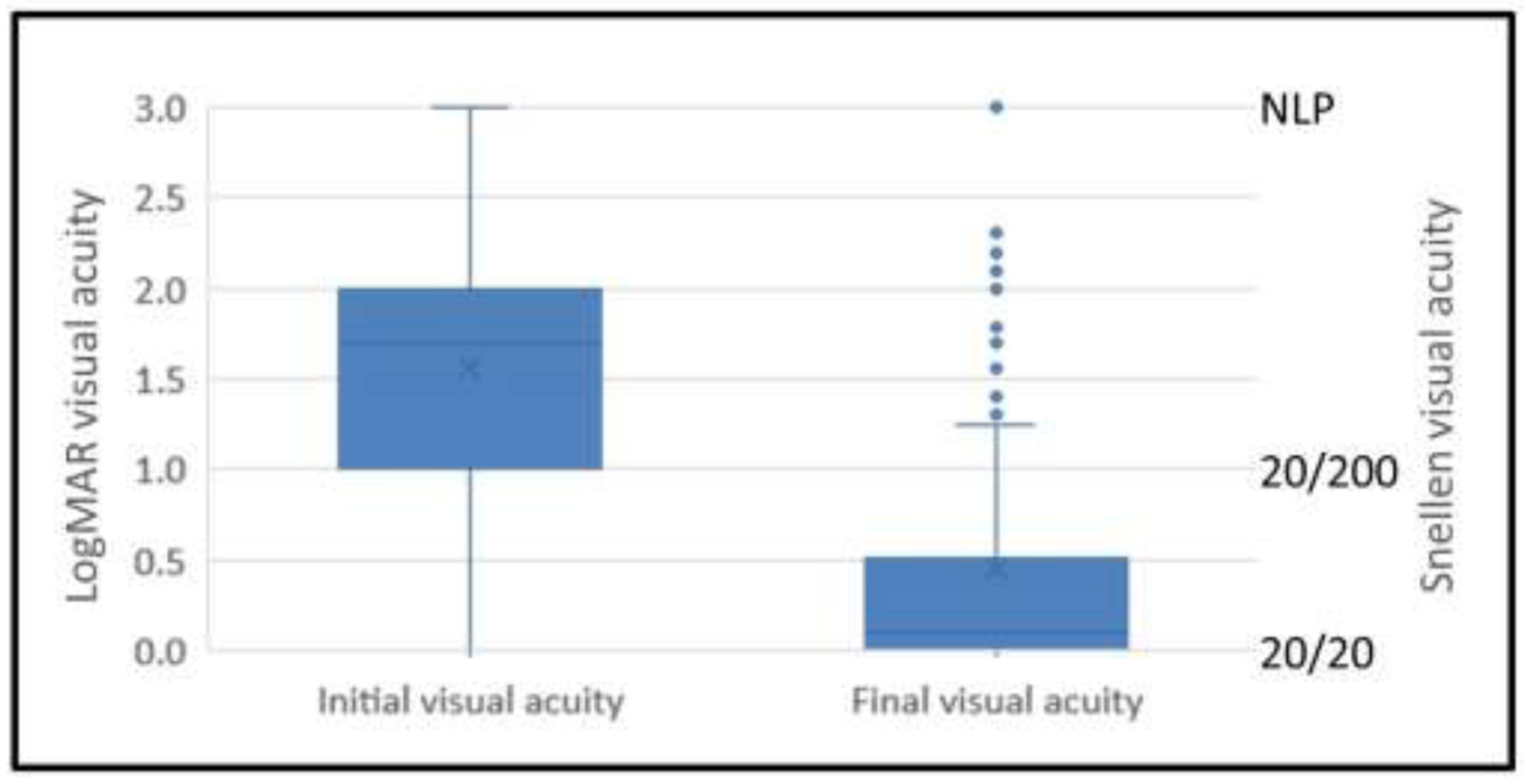
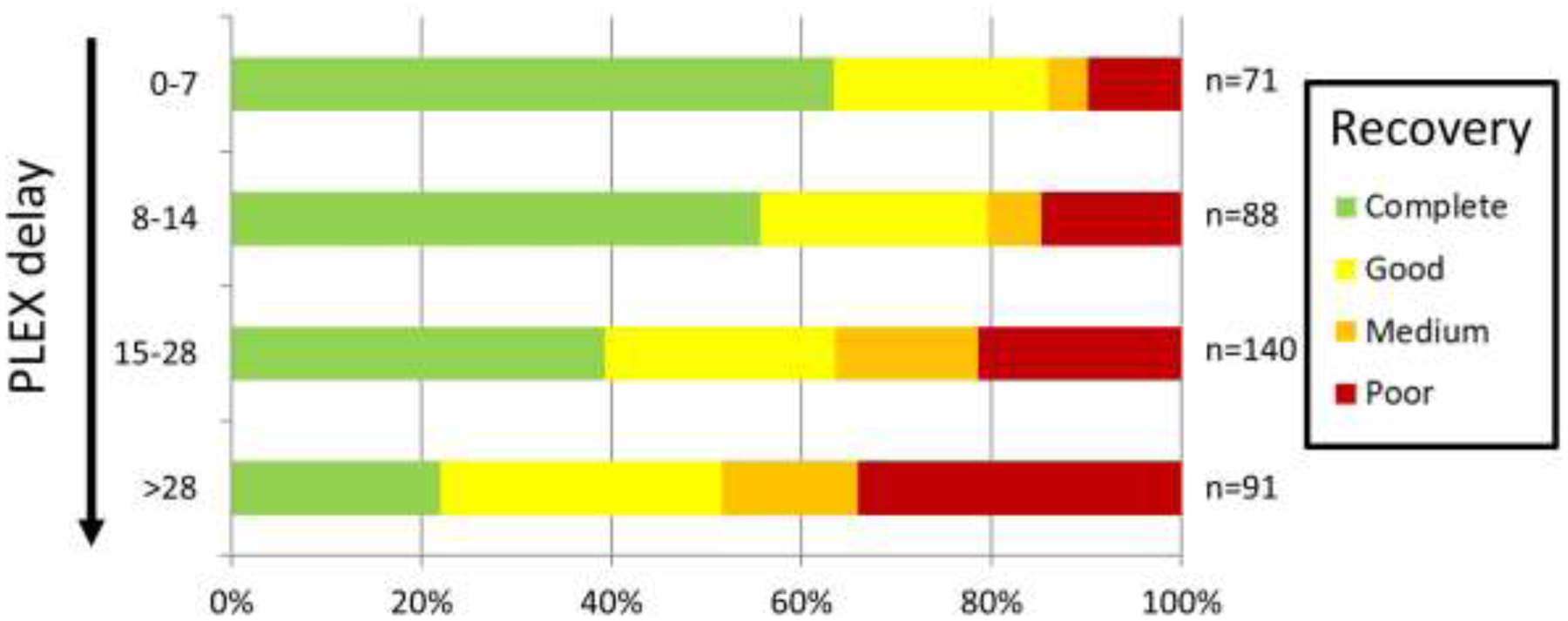
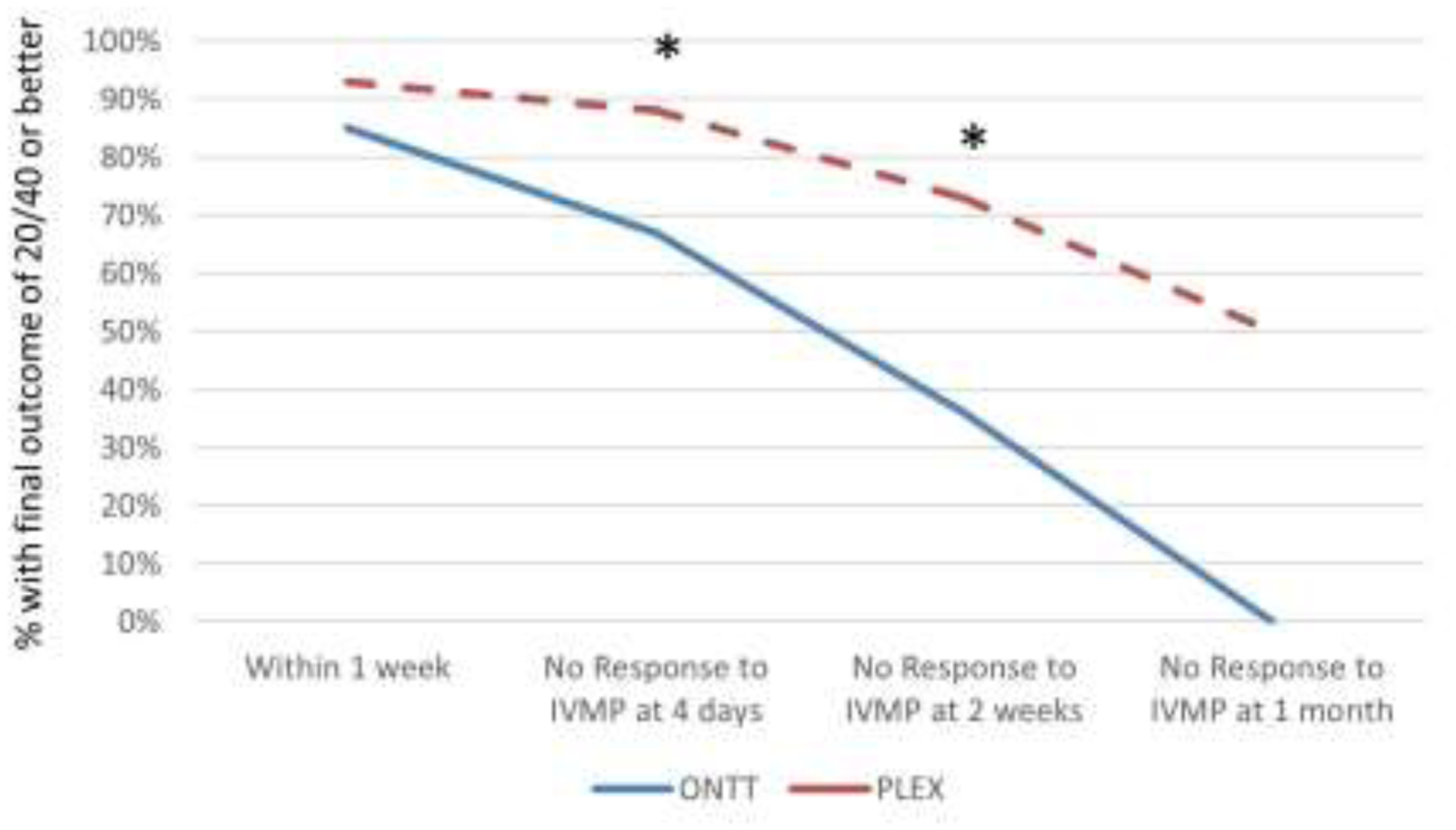
Results: A total of 395 ON attack treated with PLEX from 317 patients were evaluated. The median age was 37 years (range 9-75), and 71% were female. Causes of ON included multiple sclerosis (108), myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) (92), aquaporin-4-IgG-positive neuromyelitis optica spectrum disorder (AQP4+NMOSD) (75), seronegative-NMOSD (34), idiopathic (83), and other (3). Median time from onset of vision loss to PLEX was 2.6 weeks (interquartile range [IQR], 1.4-4.0). Median visual acuity (VA) at the time of PLEX was count fingers (IQR, 20/200-hand motion), and median final VA was 20/25 (IQR, 20/20-20/60) with no differences among etiologies except MOGAD-ON, which had better outcomes. In 81 (20.5%) ON attacks, the final VA was 20/200 or worse. Patients with poor outcomes were older (P = .002), had worse VA at the time of PLEX (P < .001), and longer delay to PLEX (P < .001). In comparison with the ONTT subset with severe corticosteroid-unresponsive ON, a final VA of worse than 20/40 occurred in 6 of 50 (12%) PLEX-treated ON vs 7 of 19 (37%) from the ONTT treated with intravenous methylprednisolone without PLEX (P = .04).
Conclusion: Most ON attacks improved with PLEX, and outcomes were better than attacks with similar severity in the ONTT. The presence of severe vision loss at nadir, older age, and longer delay to PLEX predicted a worse outcome whereas MOGAD-ON had a more favorable prognosis. NOTE: Publication of this article is sponsored by the American Ophthalmological Society.
Copyright © 2023 Elsevier Inc. All rights reserved.
Figures
References
-
- Toosy AT, Mason DF, Miller DH. Optic neuritis. Lancet Neurol 2014;13:83–99. - PubMed
-
- Bennett JL, Costello F, Chen JJ, et al. Optic neuritis and autoimmune optic neuropathies: advances in diagnosis and treatment. Lancet Neurol 2022. - PubMed
-
- Beck RW, Cleary PA, Anderson MM Jr., et al. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N Engl J Med 1992;326:581–8. - PubMed
-
- Chen JJ, Pittock SJ, Flanagan EP, Lennon VA, Bhatti MT. Optic neuritis in the era of biomarkers. Surv Ophthalmol 2020;65:12–7. - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–12. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
