

Inhaled anti-TSLP antibody fragment, ecleralimab, blocks responses to allergen in mild asthma
- PMID: 36822634
- PMCID: PMC9996823
- DOI: 10.1183/13993003.01193-2022
Inhaled anti-TSLP antibody fragment, ecleralimab, blocks responses to allergen in mild asthma
Abstract
Background: Thymic stromal lymphopoietin (TSLP) is a key upstream regulator driving allergic inflammatory responses. We evaluated the efficacy and safety of ecleralimab, a potent inhaled neutralising antibody fragment against human TSLP, using allergen inhalation challenge (AIC) in subjects with mild atopic asthma.
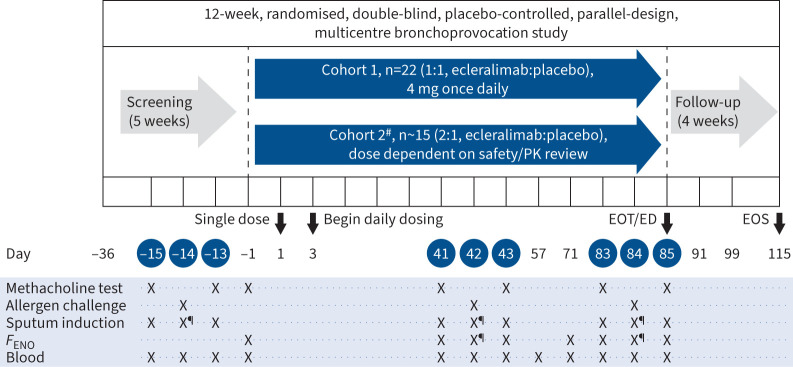
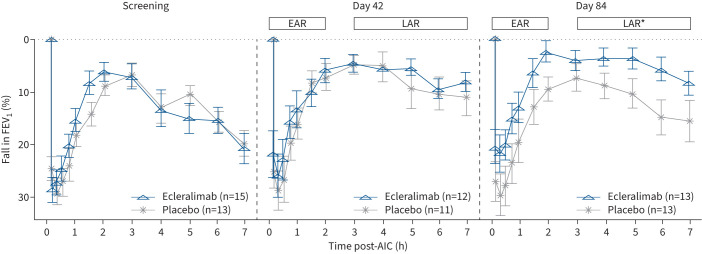
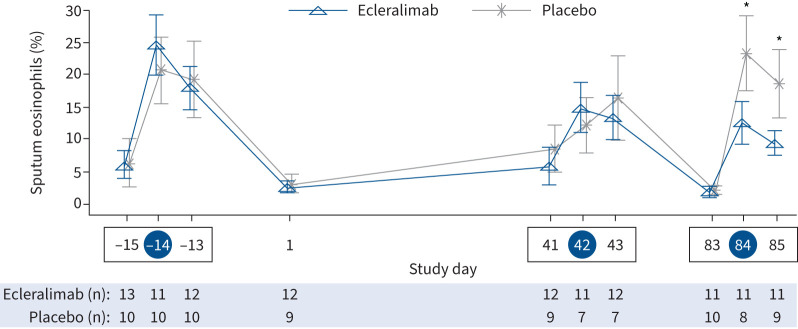
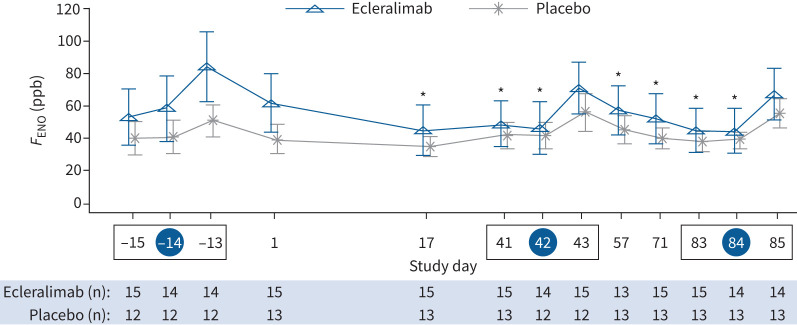
Methods: This was a 12-week, randomised, double-blind, placebo-controlled, parallel-design, multicentre allergen bronchoprovocation study conducted at 10 centres across Canada and Germany. Subjects aged 18-60 years with stable mild atopic asthma were randomised (1:1) to receive 4 mg once-daily inhaled ecleralimab or placebo. Primary end-points were the allergen-induced change in forced expiratory volume in 1 s (FEV1) during the late asthmatic response (LAR) measured by area under the curve (AUC3-7h) and maximum percentage decrease (LAR%) on day 84, and the safety of ecleralimab. Allergen-induced early asthmatic response (EAR), sputum eosinophils and fractional exhaled nitric oxide (F ENO) were secondary and exploratory end-points.
Results: 28 subjects were randomised to ecleralimab (n=15) or placebo (n=13). On day 84, ecleralimab significantly attenuated LAR AUC3-7h by 64% (p=0.008), LAR% by 48% (p=0.029), and allergen-induced sputum eosinophils by 64% at 7 h (p=0.011) and by 52% at 24 h (p=0.047) post-challenge. Ecleralimab also numerically reduced EAR AUC0-2h (p=0.097) and EAR% (p=0.105). F ENO levels were significantly reduced from baseline throughout the study (p<0.05), except at 24 h post-allergen (day 43 and day 85). Overall, ecleralimab was safe and well tolerated.
Conclusion: Ecleralimab significantly attenuated allergen-induced bronchoconstriction and airway inflammation, and was safe in subjects with mild atopic asthma.
Trial registration: ClinicalTrials.gov NCT03138811.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: G.M. Gauvreau reports grants and personal fees from AstraZeneca, and grants from Biohaven, Genentech and BioGaia, outside of the submitted work. J.M. Hohlfeld reports grants from Novartis AG, during the conduct of the study; grants from AltamiraPharma GmbH, Astellas Pharma GmbH, AstraZeneca AB, Bayer AG, Beiersdorf AG, Boehringer Ingelheim Pharma GmbH & Co. KG, CSL Behring GmbH, Desitin Arzneimittel GmbH, F. Hoffmann-La Roche AG, Genentech, Inc., GlaxoSmithKline GmbH & Co. KG, Janssen Pharmaceuticals NV, M&P Pharma AG, Novartis AG, Sanofi-Aventis Deutschland GmbH and UCB Pharma GmbH and personal fees from Boehringer Ingelheim Pharma GmbH & Co. KG, CSL Behring GmbH, Merck & Co, Inc., Nocion Therapeutics, Inc., HAL Allergy Group and Novartis AG, outside of the submitted work. M.J. FitzGerald reported receipt of research funding from Novartis which was paid directly to UBC for the completion of this study and has also been in receipt of AllerGen CIHR and NIH grant funding unrelated to the current study. L-P. Boulet reports receiving grants from Amgen, AstraZeneca, GlaxoSmithKline, Merck, Novartis and Sanofi-Regeneron, personal fees from AstraZeneca, GlaxoSmithKline, Merck, Novartis and Sanofi-Regeneron, and honoraria for lectures, presentations, speaker bureaus, manuscript writing or educational events, outside of the submitted work. D.W. Cockcroft reports receiving grants from the Department of Medicine University of Saskatchewan, AstraZeneca, Novartis, CSACI and AllerGen NCE, outside of the submitted work. B.E. Davis has nothing to declare. S. Korn reports receiving personal fees from Novartis, outside of the submitted work. O. Kornmann reports receiving personal fees from Sanofi, Novartis, Boehringer Ingelheim, Adagio, AstraZeneca, Santhera and Chiesi, outside of the submitted work. R. Leigh reports receiving personal fees from Novartis, AstraZeneca, GlaxoSmithKline, Sanofi Genzyme and Valeo Pharma Inc., outside of the submitted work. I. Mayers has nothing to declare. H. Watz reports receiving grants and personal fees from Novartis, AstraZeneca, GlaxoSmithKline, Chiesi and Boehringer Ingelheim, outside of the submitted work. S.S. Grant, M. Jain and P.E. Pertel are employees of Novartis Institutes of Biomedical Research. M. Cabanski was an employee of Novartis during the time of the study. I. Jones and J.R. Lecot are employees of Novartis Pharma AG. H. Cao is an employee of Novartis Pharmaceuticals Corporation. P.M. O'Byrne has obtained grants in aid of research from Novartis for the conduct of the current study, as well as from AstraZeneca, Medimmune, Biohaven, Merck and Bayer for research outside the current study, and received personal fees for consulting or speaker fees from AstraZeneca, GSK, Medimmune, Chiesi, Menarini and Covis.
Figures
Comment in
-
Local targeting of TSLP: feat or defeat.Eur Respir J. 2023 Mar 9;61(3):2202389. doi: 10.1183/13993003.02389-2022. Print 2023 Mar. Eur Respir J. 2023. PMID: 36894191 No abstract available.
References
-
- Mosmann TR, Cherwinski H, Bond MW, et al. . Two types of murine helper T cell clone. I. Definition according to profiles of lymphokine activities and secreted proteins. J Immunol 1986; 136: 2348–2357. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous