

Predictive biomarkers for PD-1/PD-L1 checkpoint inhibitor response in NSCLC: an analysis of clinical trial and real-world data
- PMID: 36822668
- PMCID: PMC9950975
- DOI: 10.1136/jitc-2022-006464
Predictive biomarkers for PD-1/PD-L1 checkpoint inhibitor response in NSCLC: an analysis of clinical trial and real-world data
Abstract
Background: Many biomarkers have been proposed to be predictive of response to anti-programmed cell death protein-1 (PD-1)/anti-programmed death ligand-1 (PD-L1) checkpoint inhibitors (CPI). However, conflicting observations and lack of consensus call for an assessment of their clinical utility in a large data set. Using a combined data set of clinical trials and real-world data, we assessed the predictive and prognostic utility of biomarkers for clinical outcome of CPI in non-small cell lung cancer (NSCLC).
Methods: Retrospective cohort study using 24,152 patients selected from 71,850 patients with advanced NSCLC from electronic health records and 9 Roche atezolizumab trials. Patients were stratified into high and low biomarker groups. Correlation with treatment outcome in the different biomarker groups was investigated and compared between patients treated with CPI versus chemotherapy. Durable response was defined as having complete response/partial response without progression during the study period of 270 days.
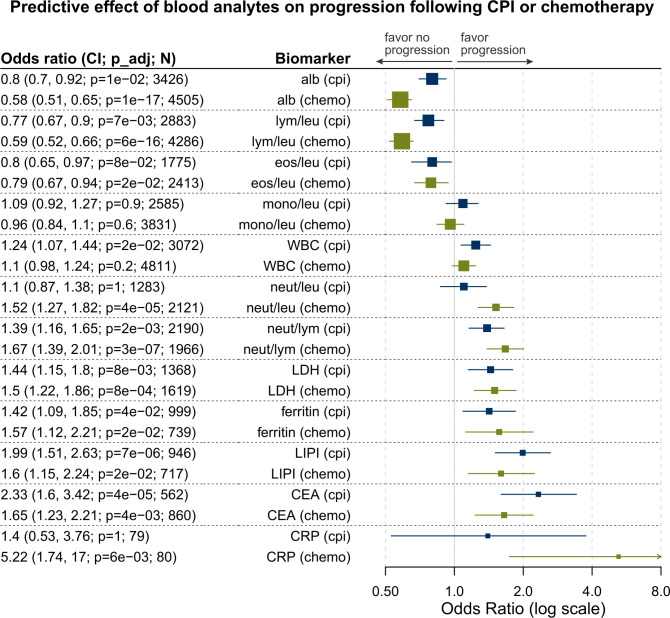
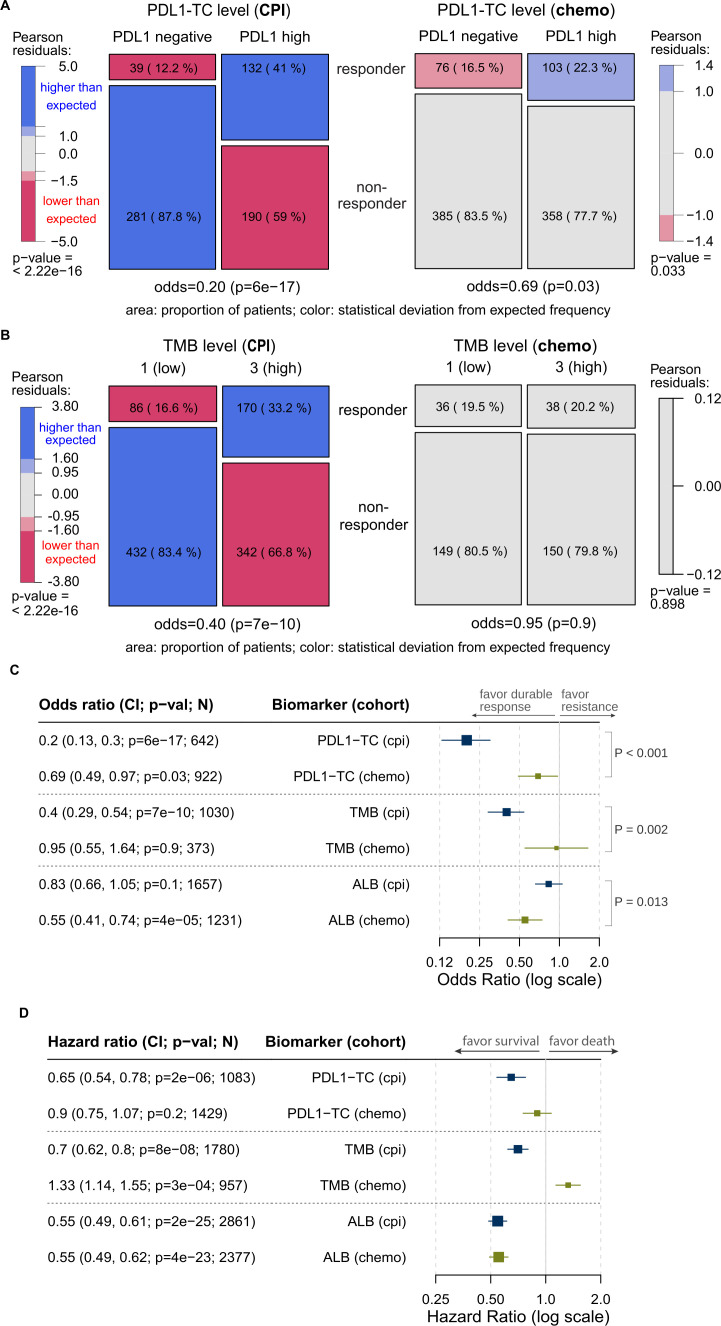
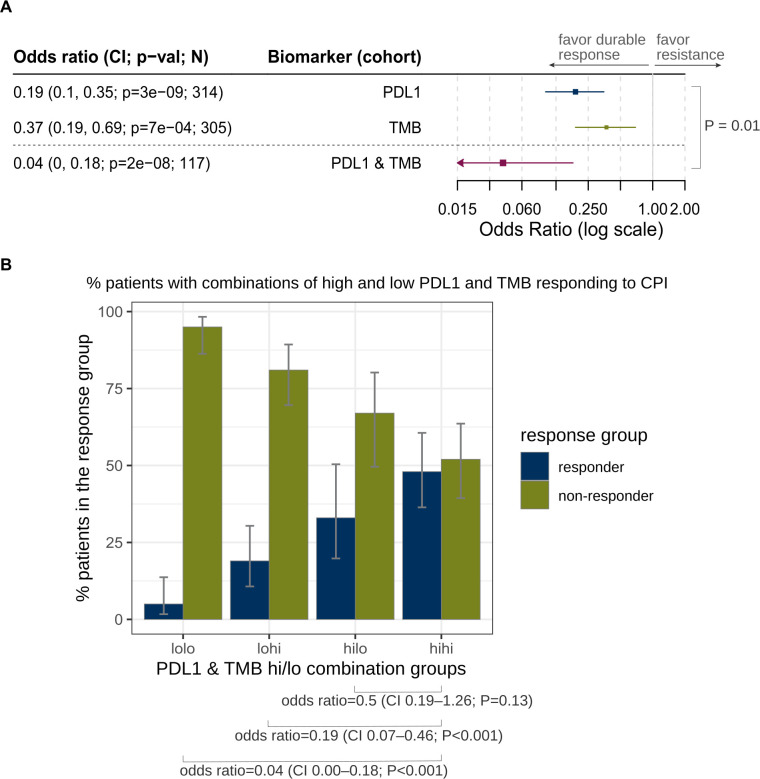
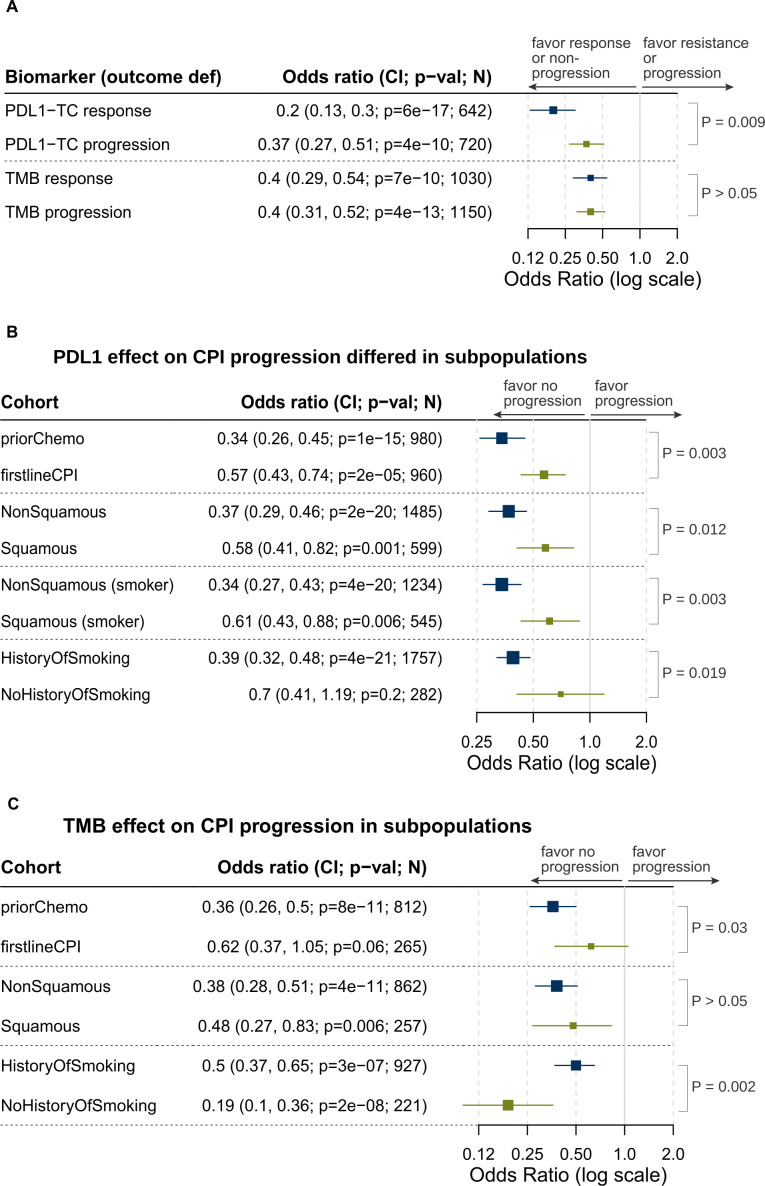
Results: Standard blood analytes (eg, albumin and lymphocyte) were just prognostic, having correlation with clinical outcome irrespective of treatment type. High expression of PD-L1 on tumors (≥50% tumor cell staining) were specifically associated with response to CPI (OR 0.20; 95% CI 0.13 to 0.30; p<0.001). The association was stronger in patients with non-squamous than squamous histology, with smoking history than non-smokers, and with prior chemotherapy than first-line CPI. Higher tumor mutational burden (TMB) (≥10.44 mut/Mb) was also specifically associated with durable response to CPI (OR=0.40; 95% CI 0.29 to 0.54; p<0.001). The combination of high TMB and PD-L1 expression was the strongest predictor of durable response to CPI (OR=0.04; 95% CI 0.00 to 0.18; p<0.001). There was no significant association between PD-L1 or TMB levels with response to chemotherapy, suggesting a CPI-specific predictive effect.
Conclusions: Standard blood analytes had just prognostic utility, whereas tumor PD-L1 and TMB specifically predicted response to CPI in NSCLC. The combined high TMB and PD-L1 expression was the strongest predictor of durable response. PD-L1 was also a stronger predictor in patients with non-squamous histology, smoking history or prior chemotherapy.
Keywords: Biomarkers, Tumor; Clinical Trials as Topic; Immunotherapy; Translational Medical Research.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Horn L, Spigel DR, Vokes EE, et al. Nivolumab versus docetaxel in previously treated patients with advanced non-small-cell lung cancer: two-year outcomes from two randomized, open-label, phase III trials (checkmate 017 and checkmate 057). J Clin Oncol 2017;35:3924–33. 10.1200/JCO.2017.74.3062 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous