

Adoption of C-reactive protein point-of-care tests for the management of acute childhood infections in primary care in the Netherlands and England: a comparative health systems analysis
- PMID: 36823597
- PMCID: PMC9947887
- DOI: 10.1186/s12913-023-09065-8
Adoption of C-reactive protein point-of-care tests for the management of acute childhood infections in primary care in the Netherlands and England: a comparative health systems analysis
Abstract
Background: The use of point of care (POC) tests varies across Europe, but research into what drives this variability is lacking. Focusing on CRP POC tests, we aimed to understand what factors contribute to high versus low adoption of the tests, and also to explore whether they are used in children.
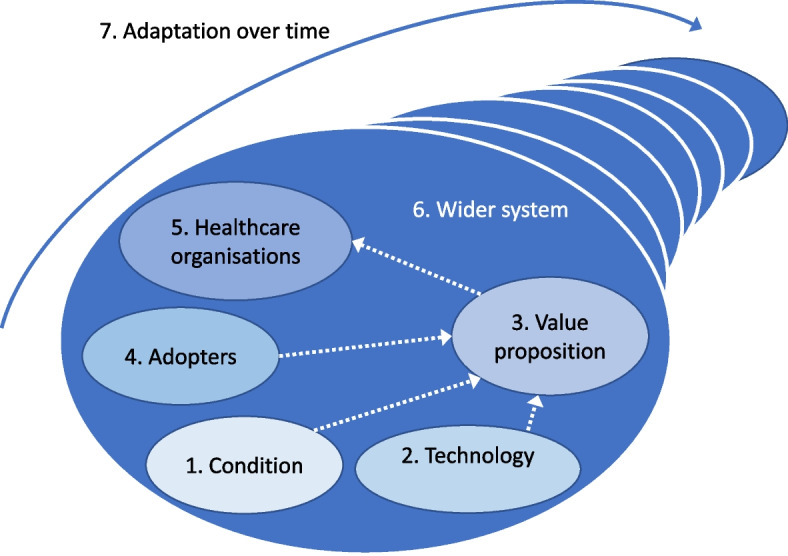
Methods: We used a comparative qualitative case study approach to explore the implementation of CRP POC tests in the Netherlands and England. These countries were selected because although they have similar primary healthcare systems, the availability of CRP POC tests in General Practices is very different, being very high in the former and rare in the latter. The study design and analysis were informed by the non-adoption, abandonment, spread, scale-up and sustainability (NASSS) framework. Data were collected through a review of documents and interviews with stakeholders. Documents were identified through a scoping literature review, search of websites, and stakeholder recommendation. Stakeholders were selected purposively initially, and then by snowballing. Data were analysed thematically.
Results: Sixty-five documents were reviewed and 21 interviews were conducted. The difference in the availability of CRP POC tests is mainly because of differences at the wider national context level. In the two countries, early adopters of the tests advocated for their implementation through the generation of robust evidence and by engaging with all relevant stakeholders. This led to the inclusion of CRP POC tests in clinical guidelines in both countries. In the Netherlands, this mandated their reimbursement in accordance with Dutch regulations. Moreover, the prevailing better integration of health services enabled operational support from laboratories to GP practices. In England, the funding constraints of the National Health Service and the prioritization of alternative and less expensive antimicrobial stewardship interventions prevented the development of a reimbursement scheme. In addition, the lack of integration between health services limits the operational support to GP practices. In both countries, the availability of CRP POC tests for the management of children is a by-product of the test being available for adults. The tests are less used in children mainly because of concerns regarding their accuracy in this age-group.
Conclusions: The engagement of early adopters combined with a more favourable and receptive macro level environment, including the role of clinical guidelines and their developers in determining which interventions are reimbursed and the operational support from laboratories to GP practices, led to the greater adoption of the tests in the Netherlands. In both countries, CRP POC tests, when available, are less used less in children. Organisations considering introducing POC tests into primary care settings need to consider how their implementation fits into the wider health system context to ensure achievable plans.
Keywords: Acute childhood infections; C-reactive protein; Comparative health systems analysis; England; NASSS framework; Point-of-care tests; Primary care; The Netherlands.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Lucas PJ, Cabral C, Hay AD, Horwood J. A systematic review of parent and clinician views and perceptions that influence prescribing decisions in relation to acute childhood infections in primary care. Scand J Prim Health Care. 2015;33(1):11–20. doi: 10.3109/02813432.2015.1001942. - DOI - PMC - PubMed
-
- WHO . World Health organization. Global action plan on antimicrobial resistance. 2015. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
