

Paediatric sepsis-associated encephalopathy (SAE): a comprehensive review
- PMID: 36823611
- PMCID: PMC9951490
- DOI: 10.1186/s10020-023-00621-w
Paediatric sepsis-associated encephalopathy (SAE): a comprehensive review
Abstract
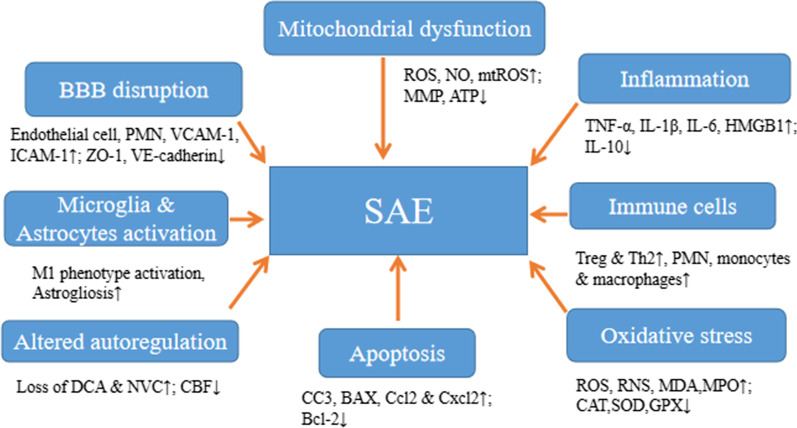
Sepsis-associated encephalopathy (SAE) is one of the most common types of organ dysfunction without overt central nervous system (CNS) infection. It is associated with higher mortality, low quality of life, and long-term neurological sequelae, its mortality in patients diagnosed with sepsis, progressing to SAE, is 9% to 76%. The pathophysiology of SAE is still unknown, but its mechanisms are well elaborated, including oxidative stress, increased cytokines and proinflammatory factors levels, disturbances in the cerebral circulation, changes in blood-brain barrier permeability, injury to the brain's vascular endothelium, altered levels of neurotransmitters, changes in amino acid levels, dysfunction of cerebral microvascular cells, mitochondria dysfunction, activation of microglia and astrocytes, and neuronal death. The diagnosis of SAE involves excluding direct CNS infection or other types of encephalopathies, which might hinder its early detection and appropriate implementation of management protocols, especially in paediatric patients where only a few cases have been reported in the literature. The most commonly applied diagnostic tools include electroencephalography, neurological imaging, and biomarker detection. SAE treatment mainly focuses on managing underlying conditions and using antibiotics and supportive therapy. In contrast, sedative medication is used judiciously to treat those showing features such as agitation. The most widely used medication is dexmedetomidine which is neuroprotective by inhibiting neuronal apoptosis and reducing a sepsis-associated inflammatory response, resulting in improved short-term mortality and shorter time on a ventilator. Other agents, such as dexamethasone, melatonin, and magnesium, are also being explored in vivo and ex vivo with encouraging results. Managing modifiable factors associated with SAE is crucial in improving generalised neurological outcomes. From those mentioned above, there are still only a few experimentation models of paediatric SAE and its treatment strategies. Extrapolation of adult SAE models is challenging because of the evolving brain and technical complexity of the model being investigated. Here, we reviewed the current understanding of paediatric SAE, its pathophysiological mechanisms, diagnostic methods, therapeutic interventions, and potential emerging neuroprotective agents.
Keywords: Apoptosis; Blood–brain barrier; Central nervous system; Cerebral autoregulation; Oxidative stress; Paediatrics; Pro-inflammatory cytokines; Sepsis; Sepsis-associated encephalopathy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effects of hydrogen-rich saline in neuroinflammation and mitochondrial dysfunction in rat model of sepsis-associated encephalopathy.J Transl Med. 2022 Nov 26;20(1):546. doi: 10.1186/s12967-022-03746-4. J Transl Med. 2022. PMID: 36435787 Free PMC article.
-
Exploring Neuroprotective Agents for Sepsis-Associated Encephalopathy: A Comprehensive Review.Int J Mol Sci. 2023 Jun 28;24(13):10780. doi: 10.3390/ijms241310780. Int J Mol Sci. 2023. PMID: 37445958 Free PMC article. Review.
-
Sepsis-associated encephalopathy and septic encephalitis: an update.Expert Rev Anti Infect Ther. 2021 Feb;19(2):215-231. doi: 10.1080/14787210.2020.1812384. Epub 2020 Sep 14. Expert Rev Anti Infect Ther. 2021. PMID: 32808580 Review.
-
Sepsis-associated encephalopathy: Mechanisms, Diagnosis, and Treatments update.Int J Biol Sci. 2025 Apr 28;21(7):3214-3228. doi: 10.7150/ijbs.102234. eCollection 2025. Int J Biol Sci. 2025. PMID: 40384873 Free PMC article. Review.
-
What's new on septic encephalopathy? Ten things you need to know.Minerva Anestesiol. 2023 Mar;89(3):217-225. doi: 10.23736/S0375-9393.22.16689-7. Epub 2022 Jul 14. Minerva Anestesiol. 2023. PMID: 35833857
Cited by
-
The effect of different dosage of intranasal dexmedetomidine on preventing emergence delirium or agitation in children: A network meta-analysis of randomized controlled trials.PLoS One. 2024 Sep 6;19(9):e0304796. doi: 10.1371/journal.pone.0304796. eCollection 2024. PLoS One. 2024. PMID: 39240955 Free PMC article.
-
Amide Proton Transfer-Weighted MR Imaging and Signal Variations in a Rat Model of Lipopolysaccharide-Induced Sepsis-Associated Encephalopathy.Metabolites. 2025 Jul 9;15(7):465. doi: 10.3390/metabo15070465. Metabolites. 2025. PMID: 40710565 Free PMC article.
-
Septic encephalopathy in the elderly - biomarkers of potential clinical utility.Front Cell Neurosci. 2023 Sep 7;17:1238149. doi: 10.3389/fncel.2023.1238149. eCollection 2023. Front Cell Neurosci. 2023. PMID: 37744876 Free PMC article. Review.
-
Diagnostic value of the combined detection of serum tumor necrosis factor-α and fecal calprotectin in early sepsis-related encephalopathy.Front Med (Lausanne). 2025 Jun 2;12:1598624. doi: 10.3389/fmed.2025.1598624. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40529149 Free PMC article.
-
High-concentration hydrogen inhalation mitigates sepsis-associated encephalopathy in mice by improving mitochondrial dynamics.CNS Neurosci Ther. 2024 Sep;30(9):e70021. doi: 10.1111/cns.70021. CNS Neurosci Ther. 2024. PMID: 39258790 Free PMC article.
References
-
- Andonegui G, Zelinski EL, Schubert CL, Knight D, Craig LA, Winston BW, Spanswick SC, Petri B, Jenne CN, Sutherland JC, Nguyen R, Jayawardena N, Kelly MM, Doig CJ, Sutherland RJ, Kubes P. Targeting inflammatory monocytes in sepsis-associated encephalopathy and long-term cognitive impairment. JCI Insight. 2018;3(9):e99364. doi: 10.1172/jci.insight.99364. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
